
We have a problem with Application Fever. The question is, what do we do about it?
The nature of the problem
Although I’ve written about this before (here and here), let me set out three points as a foundation.
1. Medical students are applying to more and more residency programs.

Yes, you read the y-axis correctly. The average U.S. medical graduate applies to 65 programs. The average international medical graduate (IMG) applies to 137.
As residency program directors (PDs) get buried under applications, they’re less able to evaluate candidates as individuals, and more tempted to outsource their decision making to a certain multiple-choice test of basic science.
2. Students apply to more programs than they need to.
Match rates do not improve when applications-per-candidate climb higher and higher. (The recent increase in match rates for IMGs is driven by an increase in number of available positions.)
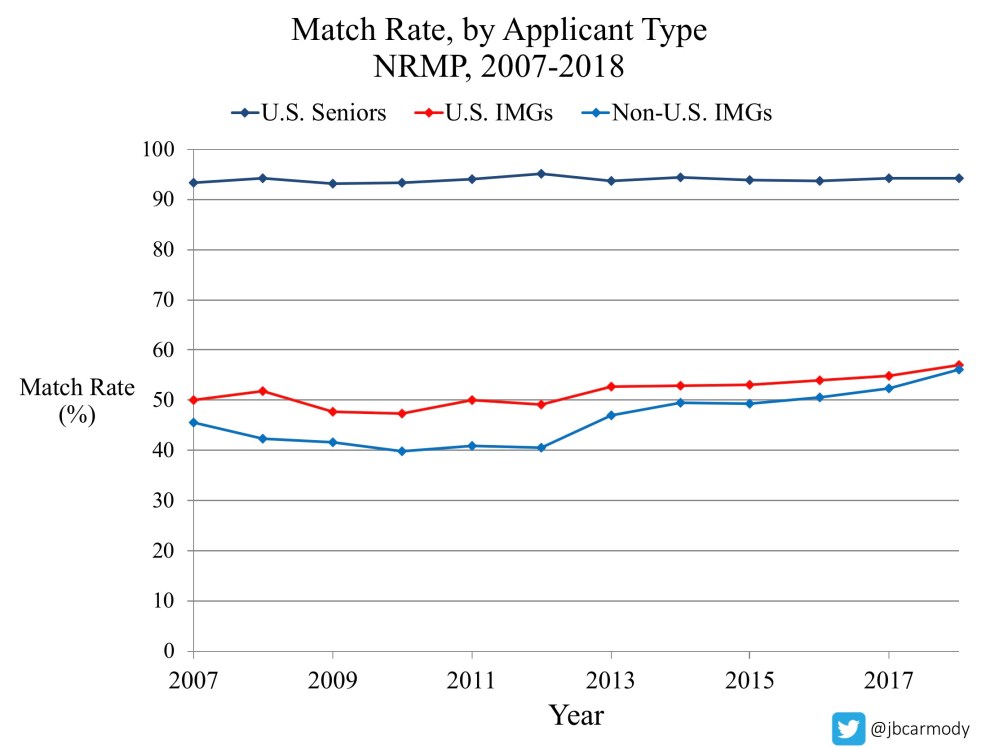
Note, however, that overapplication does increase the relative likelihood that an individual student will match. (Unfortunately, as applications climb, students have to apply to more programs to achieve a relative advantage over their peers.)
3. Overapplication benefits its corporate sponsor.
Application Fever has been quite beneficial for the Association of American Medical Colleges (AAMC), sponsor of the Electronic Residency Application System (ERAS).

In 2019, the AAMC took in $94,153,946 in revenue from ERAS alone – far more than it generated from any of its other programs (including the MCAT, AMCAS, and membership dues).
_
So what do we do about all this?
If the current system benefits neither PDs nor students, then why do we tolerate it? How do get out from under this?
There are two broad strategies. We can impose external limits (“caps”), or we can try to improve marketplace efficiencies/incentives to reduce overapplication.
Let’s take a look at how some particular strategies might work, considering the pros, cons, and likely unintended consequences.
_
Part I: Caps
There are a few possible variations.
1. Application Caps
The idea
Instead of applying to as many programs as they want, applicants can only apply to a certain number (say, 20 programs).
The good
Application Fever will be over.
The bad
There are a couple of things.
First, there’s something vaguely un-American about application caps. We live in a country where part of our ethos is that you’re allowed to have as much of something as you can pay for. (Of course, you can argue that the Match process itself is un-American. In fact, it would have been overturned for violating antitrust laws had Congress not specifically amended the U.S. Code to allow it).
Second, application caps put the burden on students to select programs that are a good fit. But do we really provide them enough data to do so intelligently?
Many programs advertise themselves in such a generic way that it’s hard for students to tell them apart (except by their geographic location and U.S. News & World Report ranking). For application caps to work well, programs have to communicate what makes them unique – and be more transparent about their selection criteria – so that candidates can figure out if they’re a good fit before they spend one of their applications.
The ugly
Although most candidates will have the same Match outcome whether they apply to 15 programs or 150, marginal candidates probably do need to apply to a lot of programs to find a home.
Therefore, if we use hard caps, we need to be prepared for more candidates to go unmatched and more programs to be unfilled. We’d have to support both groups through a destigmatized, fair, and efficient SOAP (the supplemental offer and acceptance program; formerly known as the “scramble”).
_
2. Program Caps
The idea
Programs directors are given the ability to limit the number of applications they review.
You only have time to read 200 applications? That’s cool. ERAS will stop sending you applications once you’ve received that many.
The good
Likely to result in holistic review. Instead of burying PDs in an avalanche of applications and forcing them to rely on a convenience metric, this would result in a manageable number of applications for PDs to carefully review.
Compared to application caps – where students may be tempted to disproportionately use their limited applications applying to the “top 20” programs – capping programs once they’ve received enough applications should result in a broader distribution of applications across all programs, and may therefore improve the Match rate.
The bad
If 1000 applicants wanted to apply to Program X, but their program is capped at 200, how would we decide which 200 get to apply?
A first-come, first served approach will result in a mad rush for students to apply as soon as ERAS opens each year. The consequences of this are entirely predictable: computers crashing, wailing, gnashing of teeth.
The ugly
There’s no guarantee that the first applicants to apply will be the best applicants. If PDs feel like they’re not getting the candidates they want, they’ll ask to increase their caps – and it won’t be long till we’re right back where we started.
_
3. Interview Caps
The idea
Instead of limiting the number of programs to which candidates can apply, or the number of applications program directors can receive, we could cap the number of interview offers that each candidate can accept.
The good
For both programs and candidates, interviews are both time-consuming and expensive. Interviewing a smaller number of more interested candidates would be an improvement for both groups. (Plus, an interview cap is likely to reduce the last-minute interview cancellations that plague many PDs.)
The bad
Capping the number of interviews a candidate can accept will likely slow down the system.
Programs review applications on their own schedules. But a student may justifiably be reluctant to accept or decline an interview offer until she’s heard from every program to which she applied. Unfortunately, that means that the pace of scheduling interviews will be limited by the slowest programs to conduct their reviews.
The ugly
Interview caps will likely do almost nothing to reduce Application Fever.
After all, the realities of time and space limit already impose limits. I mean, you can apply to 100 programs if you want, but you can’t pull off 100 interviews. Students overapply (and overaccept interview offers, often to cancel with short notice), but are probably appropriately limiting their interviews now.
_
Part II: Marketplace interventions
Instead of imposing caps, we could try solutions to make the marketplace work better. We want to make it easy for students to apply to fewer programs, and harder for them to overapply. Toward that end, we could consider…
1. Tax on Excess Applications
The idea
If we want students to apply to fewer programs, one way to do that is to increase the cost of applying to so many. Beyond a certain limit, candidates could apply to more programs only by paying a “tax”.
The good
If the cost of overapplication is prohibitive, then candidates will stop applying to so many places.
The bad
To work, the tax would really have to be prohibitive.
After all, what’s the cost of finishing a four-year medical education but going unmatched in your preferred specialty? Pretty steep. And unless the cost of more applications is greater than the cost of going unmatched, rational candidates will suck it up and pay the tax.
Also, we’re kinda doing this already. The current ERAS Fee Schedule is tiered. The first 10 programs cost ~$10 apiece, with increasing costs per application until they max out at $26 for each program >30. And all this has done is put more money in the AAMC coffers.
The ugly
Paying a tax matters more to some applicants than others.
We hear a lot about rising student loan debt for medical students. In 2018, the AAMC reported that the average debt for students who took out loans was $196,520.
But the truth is that there is a bimodal distribution of indebtedness, with growing numbers of the heavily indebted students and the group of students who complete medical school with zero debt.

(Graphic from Grischkan J, et al. JAMA Intern Med 2017; 177(10): 1532-1535. PubMed)
A tax would disproportionately impact students with fewer financial resources (or less willingness to take on more debt), while financially privileged candidates would become even more advantaged in the residency selection process. If we want residency selection to be a meritocracy, this probably isn’t the way to do it.
_
2. Application Transparency
The idea
Program directors would be able to see the list of other programs to which an applicant applied.
The good
Most PDs don’t want to spend a whole lot of time rolling out the red carpet for candidates who don’t really want to match there. If they could see the other programs to which a student applied, they might get a sense of where their program might fall – and could adjust their decision to interview appropriately.
Transparency may also cut down on one of the most wasteful types of application inflation: well qualified students who apply in multiple different specialties.
As I’ve pointed out before, the ERAS Cross Specialty Applicant Data (below) are getting kind of ridiculous.
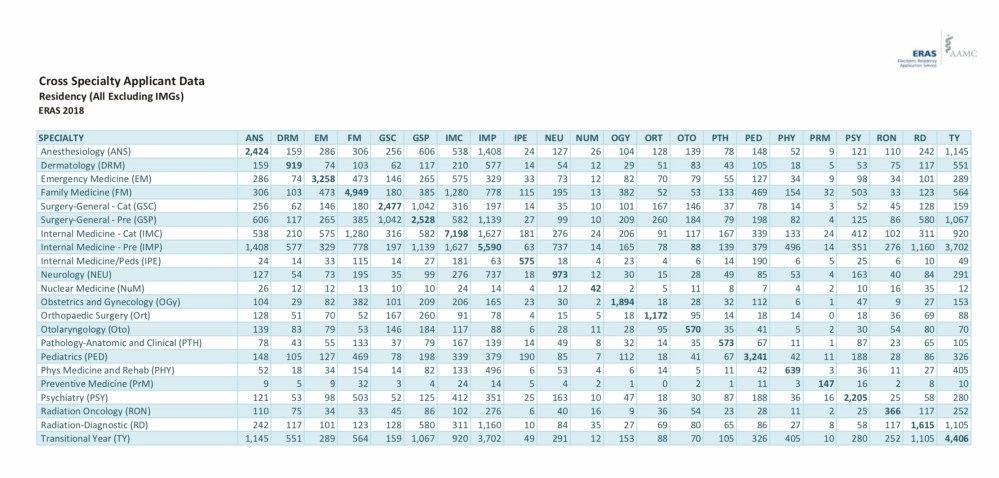
(Data for U.S. medical graduates. Each cell reflects the number of candidates who applied to programs in both specialties.)
It’s true that candidates applying in highly competitive specialties may need a backup. But it’s also true that when well-qualified candidates overapply to specialties that aren’t their first choice, it makes the process less efficient for everyone else.
The bad
Would transparency really matter?
The hope is that transparency would shame students into applying to fewer programs (or backup specialties). But if the majority of students continue applying to a ton of programs (plus a backup specialty or two), what is there to be ashamed about?
If students aren’t shamed into applying less, there’s not much else that PDs can do. Demanding that a candidate explain why he applied to programs in four different “lifestyle” specialties would probably be considered a Match violation.
Moreover, do PDs even really have the time to analyze this type of information? When I talk about #USMLEPassFail, I always hear from a few PDs who claim to have no more time to review applications than it takes for them to sort the applications by Step 1 scores in ERAS.
The ugly
If PDs decline to interview candidates for whom their program looks like a “safety school,” match rates may decrease, and some very qualified candidates will crash into the SOAP.
_
3. Extra Application Requirements
The idea
The introduction of ERAS in 1996 made the residency application process much more efficient. Instead of mailing individual applications all over the country, students could apply to any number of programs with just a click.
But maybe ERAS has made things too easy.
If programs added an extra application requirement specific to their program – say, a short essay – then maybe applications would drop.
The good
The kind of candidate who would be deterred from applying by a small extra requirement is probably a candidate who isn’t that interested in your program. This would eliminate the very applications PDs are trying to screen out anyhow.
The bad
Students will complain.
Applying to residency is already a time consuming process, and will only be made more so by having to complete a bunch of penny-ante side applications.
The ugly
Although it’s likely to work initially, I think it provide only a temporary fix.
Students may complain about the burden of side applications… but students who complete more of them will enjoy a relative advantage in the high-stakes residency selection competition. So each year, students will budget more and more time and effort to completing whatever side applications PDs are requesting. It will just be a new arms race. And like Step 1 Mania, “Side Application Mania” would probably come at the cost of disengagement from educational activities.
_
4. Preference Signaling
The idea
Applicants can designate a limited number of programs (say, 2-3) as their priority programs. This would signal to those programs a high degree of interest that may help PDs make decisions to interview.
The good
Mathematical modeling shows that it might work.
The bad
Despite the analysis linked above, I’m skeptical that this would work long term.
Why? Well, if submitting a “priority application” increases a student’s chance of getting an interview, students will quickly realize that they’ll reap the greatest benefit from these applications by spending them on their “reach” programs, whether those are truly the programs they’re most interested in or not. All it takes is a certain threshold of students who try to game the system by dumping their priority applications on the same group of elite programs, and the priority designation will stop signaling true interest and just become another screening metric used by already-overburdened PDs to reduce their application pile.
The ugly
Will it actually reduce applications overall? I’m not sure.
Priority signaling may help some candidates get interviews at their dream programs – but the existence of a tiered application system seems likely to devalue ‘non priority’ applications even further. And if each non-priority application is worth less, then you’d better submit even more of them, right? Though well-intentioned, priority signaling may encourage even more of a shotgun approach for lower value non priority applications.
_
A call to action
So which of these is the best plan?
I’m not sure.
I personally think application caps are necessary, and we should focus attention on setting a sensible limit; improving the information candidates receive from programs regarding their competitiveness; and strengthening the SOAP.
But there is one thing about which I am certain: we can’t allow Application Fever to continue on unchecked.
And there’s another thing I’m pretty certain about, too: program directors will have to lead the change.
Wait…who?
Yes, program directors.
Program directors are the ones hurt most by Application Fever. As applications increase, they’re getting crushed like a worm in a box of rocks. And while the existence of USMLE Step 1 scores gives them a mechanism to screen applications and maintain their sanity, most PDs agree that it’s not the best way to pick our future residents. They use it because they have to, and because there’s not a time-efficient alternative at the moment.
But if the problem for PDs is that they’re being buried in applications, we need to ask: is the best solution to continue to rely on a non-evidence based metric with harmful externalities, or is it do demand application reform?
Sometimes, when I make this point, I get pushback from PDs who sound like they’ve been in the experimental arm of a learned helplessness experiment. But although they may feel helpless, I’d argue that they’re the only ones who can do anything about Application Fever.
Students are powerless. Like with so many other things (cough, cough, Step 1 Mania), they’re trapped in an arms race with each other that has no natural end.
And what about the AAMC, sponsor of ERAS?
Well, if you didn’t catch the charts above, they have a financial interest in maintaining Application Fever. (In fact, they continue to put out messaging encouraging students to apply to even more programs – more on that in the future).
So no, the AAMC isn’t going to rescue us. That is, unless we make the cost of continued inaction greater than the cost of application reform.
Imagine this: a group of program directors stands together before the AAMC and says, “Look. We’re getting killed by these applications. You have three years to come up with a solution, or we’re gonna walk. If you don’t fix this, we’ll stop accepting ERAS and start using our own website, and we’ll use caps or whatever else we want.”
Sound unrealistic? I don’t think so.
Every specialty has an association of program directors. (Many of them issued official position statements on USMLE score policy.) So there is already mechanism in place for political action.
And what about the cost of starting a new application service? I don’t think it will be a problem.
ERAS is just a secure website. It’s neither unique nor irreplaceable. Actually, it doesn’t even work that well – look no further than the prolonged downtime during the 2019 SOAP.
And if you went to Silicon Valley and shopped around, I’ll bet you could find multiple developers who would build a better website for the same amount of money students are spending now on ERAS. (You might even get some VC folks interested in getting it off the ground, given the likely future growth if the new competitor is successful.)
So I don’t think that a threat to walk away from ERAS is an empty one. The question is, will anyone have the courage to stand up and demand reform?
