Last week, I Tweeted about the rapid change in emergency medicine (EM) applicants and the likelihood that many EM programs will go unfilled in this year’s Match.
In response, I got several interesting DMs – from potential applicants, current residents, EM physicians, and even a program director. Upon reflection, some of the points I made in those discussions may be useful to a broader audience.
Let’s start with the facts.

FACT: Emergency medicine was surprisingly SOAP-y in the 2022 Match.
Historically, EM has been a pretty competitive match. Over the past 15 years, ~98-100% of EM positions filled in the Match, with only a few scraps left for the SOAP. Suddenly, in 2022, there were 217 unfilled positions.
–
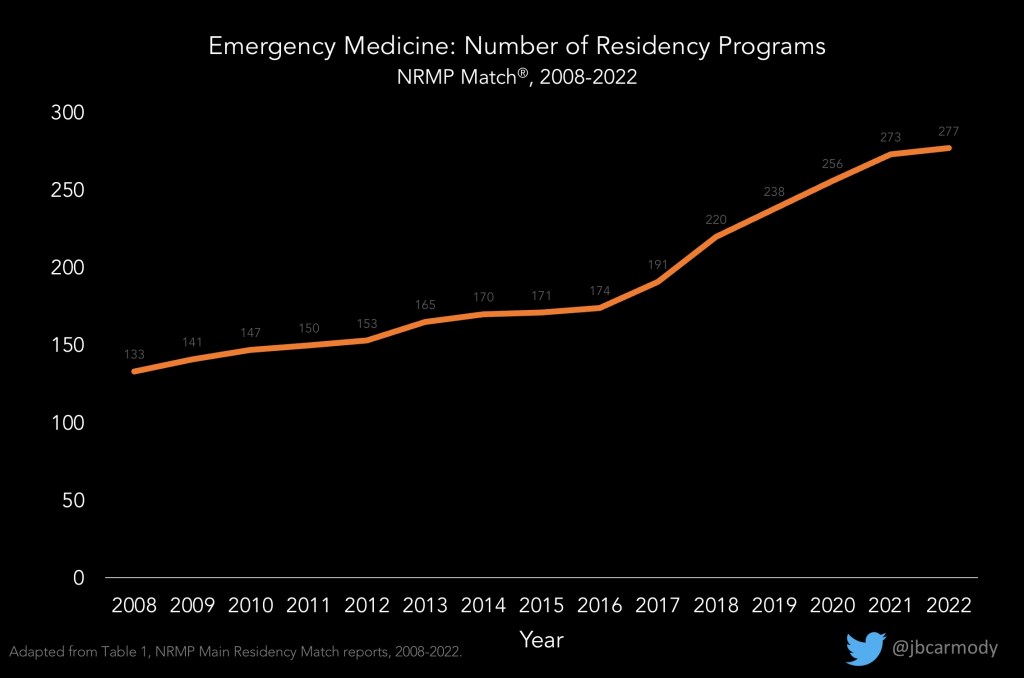
FACT: The number of emergency medicine residency programs participating in the Match has more than doubled in the past 15 years.
This is at least partially explained by the movement of osteopathic programs into the single accreditation system (note the especially rapid growth from 2016-2020). And though growth in programs may help to explain the increase in SOAP positions, focusing on this in isolation ignores another, more ominous trend.
–

FACT: The number of EM applicants declined in the 2021-2022 season.
This is the real issue. Programs are up, sure. But the decline in applicants is the proximate reason so many programs found themselves in the SOAP in 2022.
–
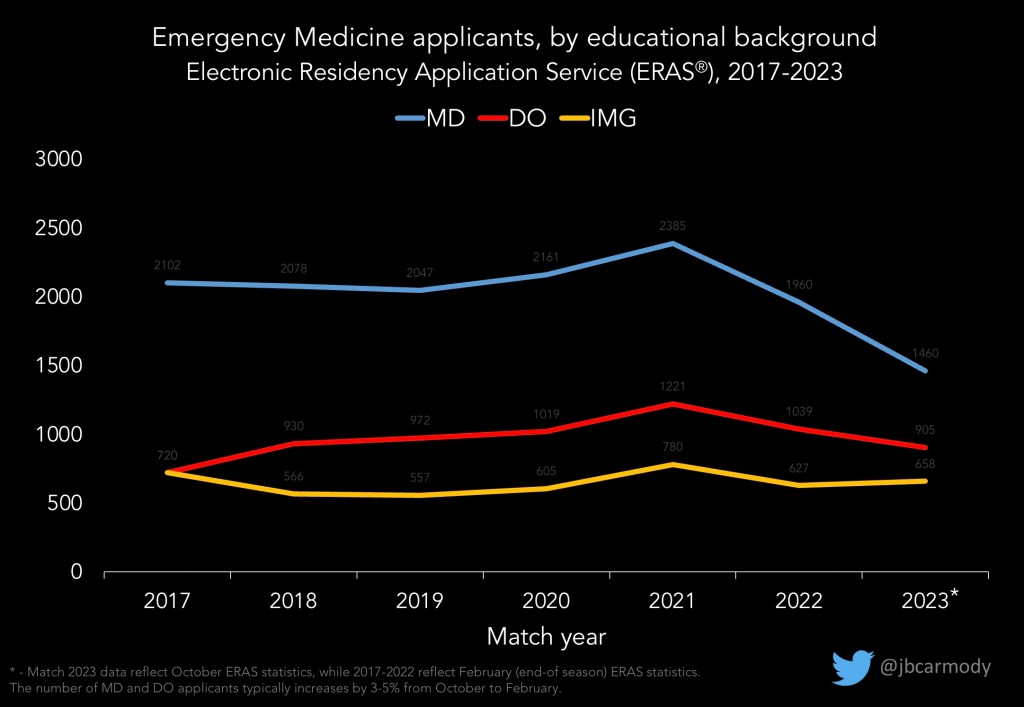
FACT: Applications are down again for 2022-2023.
There will be no rebound in EM applications – at least not this year.
Preliminary ERAS statistics show that the number of applicants from US medical schools continues to fall (down ~10% for DOs and ~25% for MDs). In other words, for many EM programs, things are gonna get worse before they get better.
–
But why are applications down?
Here’s where the facts end and conjecture begins.
Theories abound about why fewer applicants are choosing EM. Potential culprits include…
- Workforce concerns – The American College of Emergency Physicians’ workforce study projects a surplus of nearly 8000 EM physicians by 2030. (That model assumes that only 20% of ED visits will be staffed by nurse practitioners or physician assistants… if it’s more than that, that real figure may be even higher.) Who wants to go through a grueling residency training just to struggle to find a job when you’re done?
- Burnout – Sure, burnout is a concern for all specialties… but there is at least a perception that EM is especially impacted. Some prominent EM physicians have openly shared their own struggles, which is praiseworthy but may nonetheless influence students’ career decisions. Meanwhile, recent (and admittedly nonscientific) surveys put EM at the top of the burnout pile.
- COVID-19 – Maybe it was too late for students in the 2020-2021 cycle to change their career choice when COVID arrived. But applicants for the 2022 and 2022 Match may have formed their opinions about the specialty during the darkest days of the pandemic, when our EM doctors were holding the line against COVID with limited PPE. It’s not hard to imagine why they may have found other specialties more appealing.
- Compensation – Back in 2017, a report noted that EM physician salaries were up 31% even as hours worked dropped by 12%, and describes sign on bonuses of $50,000-$100,000 as not infrequent. The market over the past 5 years has certainly cooled. EM physician compensation dropped by 27% during the pandemic, and private equity firms are bragging about how they’ll increase profits by reducing physician salaries.
Obviously, these possibilities are neither mutually exclusive nor exhaustive. And it’s entirely possible that the decline in EM applicants has nothing to do with EM – it could be that ‘hot’ specialties (like anesthesiology or radiology) have just been more effectively competing for the hearts and minds of medical students over the past couple of cycles.
But regardless of why, the what is clear – there are unquestionably fewer EM applicants. So the next question is, if you care about emergency medicine, what – if anything – should you do about it?
And look, I’m not in EM. I don’t have a dog in the fight. But if you wanna know what I think – and if you turn up in my DMs, or are still reading the article at this point, I’ll presume you do – here it is.
–
MY ADVICE
…for the “meh, it’s all cyclical” guys
Look, even I’ve been around long enough to see how the popularity of specialties rise and fall.
When I graduated from medical school 15 years ago, radiation oncology had a Match rate on par with otolaryngology and orthopedic surgery, while psychiatry had the lowest mean USMLE score of any specialty and was considered a safe backup for any U.S. MD. Now, radiation oncology positions are routinely available in the SOAP, while the match rate for psychiatry is among the lowest for the nonsurgical specialties.
When you take the long view, some of the specialties that go cold get hot again. Anesthesiology is one good example. Thirty years ago, fears that anesthesiologists would be replaced by nurse anesthetists led to plummeting interest: by the late 1990s, half of anesthesiology programs didn’t fill. Yet by 2022, anesthesiology was hotter than ever, with a Match rate of 89% for graduating MD and 66% for graduating DO students.
So no, the sky is not falling. EM remains a very strong and popular specialty. Its upper echelons are as competitive as any field’s (and are likely to remain that way). And even if a couple of hundred positions go unfilled in the Match… well, we have the SOAP for a reason.
Still, the “just take the long view” argument seems a bit like climate change denialism to me. The downturn in applications from graduating U.S. MDs is precipitous and unprecedented. It is not inevitable that applicants will rebound. At the very least, the situation deserves a root cause analysis before glibly proclaiming that it’s just a blip.
–
…for EM program directors
If you don’t want your program to end up in the SOAP, you need to look closely at your international medical graduate (IMG) applicants.
Historically, that hasn’t been necessary for many EM programs: they got more than enough applicants from U.S. schools to fill their entire interview calendar. (The fact that EM was the pioneer specialty in requiring standardized letters of evaluation (SLOEs) is telling: it’s not always easy for non-U.S. MD applicants to get letters from an academic EM physician, which suggests that these groups were often an afterthought.)
But as the number of U.S. applicants decline, times are changing.

If your program wants to continue interviewing only American graduates, have at it. But remember that these applicants interview at a ton of programs: the average successful MD/DO applicant in 2022 interviewed at and ranked 16+ EM programs. So as the number of MD and DO applicants drifts down, you’ll be fighting over an increasingly scarce resource – and leaving talent on the table.
–
…for EM applicants
Don’t freak out.
Recognize that your future happiness as a physician really has nothing to do with how competitive your match was.

I say this as a pediatrician – the only specialty with a higher Match rate than EM in 2022. Matter of fact, the number of U.S. MDs who applied in pediatrics has been in decline for a decade now, yet I can assure you that fact has never impacted my day-to-day career satisfaction (which is considerable) one iota.
I dare say the same will be true for you. Show me a pediatrician or a neurosurgeon or an EM physician, and whether they love (or hate) their job will have absolutely nothing to do with how many applicants couldn’t get in when they matched. The job is what it is, and if you think it’s a good fit for you, how many of your classmates think it’s a good fit for them is completely irrelevant.
So instead of worrying about what other applicants are doing, evaluate the specialty on its merits.
And here, I’m gonna be honest, some of the concerns about EM (like the workforce data and private equity encroachment) would give me pause if I were an EM applicant. But in truth, no specialty in medicine is protected from disruptive change – especially when you’re looking at a 30+ year career. Do what you love and what you think you’re good at – and trust that if you do, you’ll be able to ride the waves even if the sea gets turbulent.
–
…for elitists and gatekeepers
If your beef is just that EM may be transitioning from a competitive to a less competitive specialty – get off your high horse.
It’s a mathematical truth that, however you define quality, half of all residents will be below average. And yet somehow, so many of them turn into outstanding clinicians and colleagues when they’re given rigorous and thoughtful training.
In graduate medical education, we waste way too much time trying to cream off the “best” residents and too little time trying to provide the best training to all residents.
And don’t smokescreen your elitism by telling me how EM patients deserve only our ‘best and brightest.’ If you’re serious about improving the quality of emergency medical care, you’ll get farther by ensuring that all residents get high-quality training than you will by trying to restrict opportunities to the select few who can bypass your ERAS filters. If your program turns out graduates who are all capable and competent, small differences when they enter aren’t really worth fighting over.
–
…for advocates
The most common question I received asked what current EM residents or physicians should do to inspire more MD/DO students to apply in EM. Beyond teaching enthusiastically, I wouldn’t waste much time on this specifically.
If the number of U.S. medical students applying in EM continues to drop, so what? The positions will fill. The only question is when (Match vs. SOAP), and by whom (US MDs vs. DOs. vs. IMGs).
In my opinion, the decline in applicants isn’t a problem per se – it’s a sign of bigger concerns. It’s like fever, or metabolic acidosis, or sinus tachycardia. It’s just an outward manifestation of internal problems, and it’s best managed not by treating it directly, but by addressing the underlying cause.
So don’t focus on the number of applicants – focus on the root problems. Seize the opportunity to broadly examine EM training and practice and focus your advocacy on things that will improve the specialty overall.
Insist that all residents receive high-quality training. Require that any new programs meet high standards for faculty supervision and clinical exposure. Demand safe staffing ratios and adequate capacity in all EDs. Ensure electronic medical records improve efficiency and patient care. Use your advocacy energy and political capital to leverage change and ease the pressure points that threaten EM more broadly – and the applicants will come.
–
ADDENDUM:
If you’d prefer a video version of this post to watch or share, there’s one at the Sheriff of Sodium YouTube site.
–
YOU MIGHT ALSO LIKE:
Match Day 2022: Winners & Losers Edition
The Residency Selection Arms Race, Part 3: The Research Arms Race
