The letters have been opened, and the 2022 Match is in the books. You know what that means…
Yeah, that’s right. It’s time to break it down, Winners & Losers style.
–
WINNER: The NRMP.
Of all the figures I wanted to see from this year’s match, the one I most wanted to see was the match rate.
Last year, match rates for both graduating U.S. MDs and DOs were down slightly from recent averages (92.8% and 89.1%, respectively). Of course, last year’s application cycle was thoroughly disrupted by COVID-19 and all that came along with it. So I wondered: would match rates rebound in 2022?
They did.
The match rate for DOs reached an all time high at 91.3%. Meanwhile, MDs matched at a 92.9% clip, which is down somewhat from the recent high water mark of 94.3% in 2018, but virtually identical to last year. The match rates for international medical graduates (IMGs) were 61.4% for U.S. citizens and 58.1% for non-U.S. citizens, and both of those figures are also up from 2021, when they were 59.5% and 54.8%, respectively (though trends in IMG match rates are hard to interpret because the number of applicants fluctuates significantly from year to year.)
Improving match rates suggest that the lower figures last year were a one-off as applicants and programs adjusted to a virtual application process. Had rates continued to decline, the matching process itself might have faced scrutiny – so count this as a big win for the NRMP.
–
LOSER: Emergency medicine programs.
The big story of Match Week was the 219 unfilled emergency medicine positions up for grabs in the SOAP. (In most recent years, there have been 20 or fewer.)
What happened?
For one thing, fewer applicants applied to EM this year. Final figures from ERAS showed a 17% drop in EM applicants versus last year.
Why were EM applicants down? It’s tempting to blame COVID – after all, the Class of 2022 spent the entirety of their final two years of medical school under the cloud of the pandemic. But other front-line specialties like internal medicine saw steady application numbers.
Instead, the biggest culprit is likely the perception of a weakening job market for emergency physicians. Last year, a highly-publicized workforce study by the American College of Emergency Physicians concluded that there could be a surplus of EM doctors by as early as 2030.
But even that’s not the full story.
The NRMP’s press release notes that this year’s EM applicants submitted shorter rank order lists than in the past – which, in context with the SOAP numbers, may suggest that the smaller pool of applicants was targeting the same segment of programs. (Many of the unfilled EM positions were offered by newer programs, often those sponsored by for-profit entities like HCA Healthcare – so these programs may have to significantly re-tool their recruitment approach if the number of EM applicants continues to decline in the future.)
–
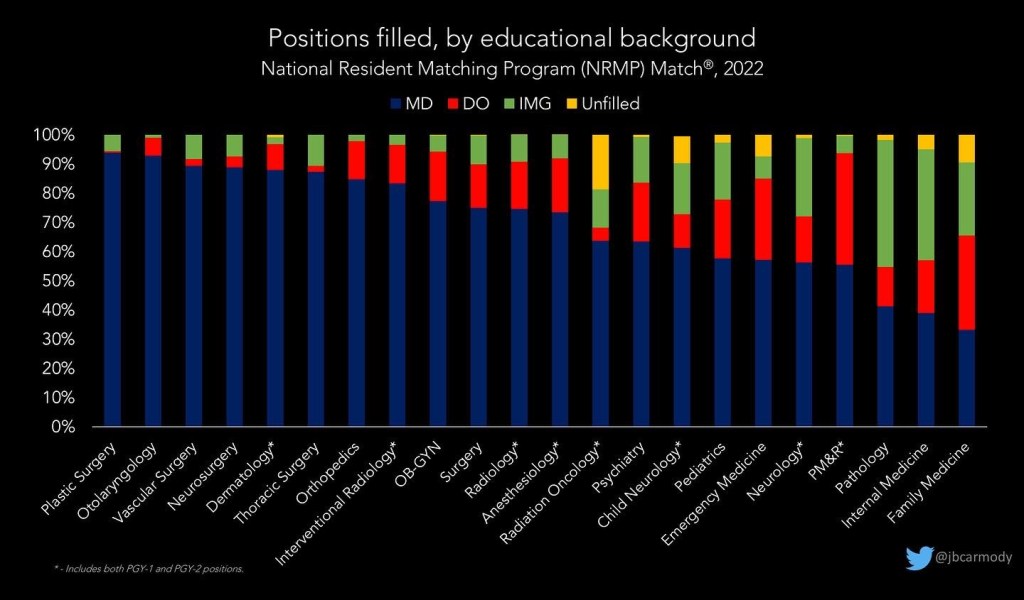
WINNER: Surgical specialties.
Perhaps unsurprisingly, it was another banner year for the most competitive (and highest-paying) surgical subspecialties. Every single position in neurosurgery, orthopedics, otolaryngology, and vascular/thoracic/plastic surgery was filled in the Match.
We won’t know the exact match rates by specialty until the NRMP releases the new Charting Outcomes reports in a few months. (That’s because the preliminary data don’t account for applicants who apply in multiple specialties. However, unless you analyze by an applicant’s preferred specialty, it’s impossible to know whether an applicant to a particular specialty was completely unmatched – or didn’t match in that specialty because they successfully matched into a more preferred specialty.) Still, just eyeballing the numbers, I think we’re going to see record low match rates in orthopedics, plastic surgery, and possibly otolaryngology, with U.S. senior match rates <70% in each field.
Meanwhile, the majority of the categorical positions left over for the SOAP were in (lower paying) primary care specialties and emergency medicine.

However, the categorical specialty with the greatest proportion of unfilled positions was again radiation oncology. (The rapid transformation of radiation oncology from among the most difficult-to-Match specialties to the one with the most unmatched positions seems to be the result of simultaneous program expansion and adverse job market forecasts, and is expertly described elsewhere.)
–
WINNER: The guy whose USMLE scores got “lost” by Prometric.
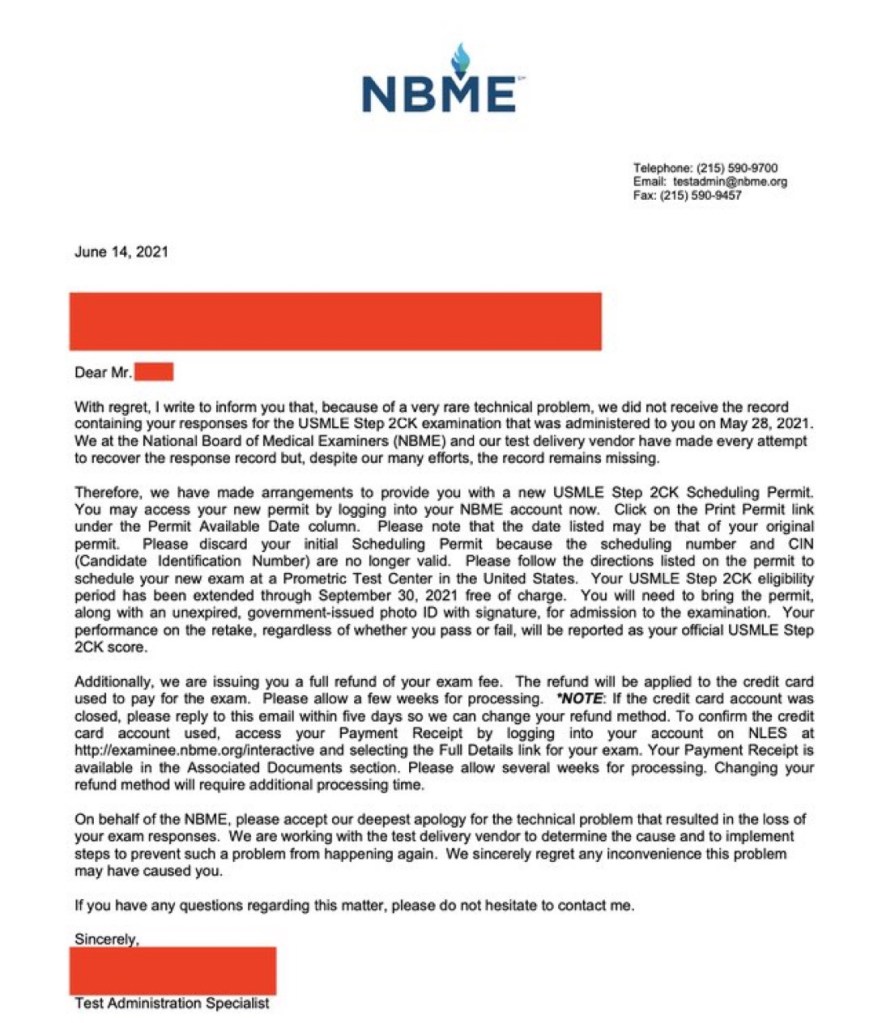
Remember this story from the beginning of the application season? An applicant took USMLE Step 2 CK, only to have his scores lost by Prometric – an organization whose single essential business function is to record test scores. And this was only the beginning of a series of unfortunate events that conspired to jeopardize the student’s chance of getting into a residency program (and culminated in legal action and advocacy from a sitting United States Senator). But last week, I learned that he matched. So at least the story has a happy ending.
–
LOSER: USMLE Step 2 CS
How could Step 2 CS lose any more? I mean, the thing was cancelled permanently a year ago!
Still, for the second year in a row, programs have evaluated applicants without Step 2 CS scores… and I didn’t hear any complaining. Even for international medical graduates, the ECFMG’s mini-CEX seems to have effectively outsourced… well, whatever it was that we used to claim USMLE Step 2 CS measured.
Although Step 2 CS is gone for good, the way we view these clinical skills examinations still has implications for the National Board of Osteopathic Medical Examiners (NBOME), who still asserts that their COMLEX-USA Level 2-PE test isn’t gone for good, just “postponed indefinitely.”
(I’m on record as predicting that Level 2-PE will return later this year…so you can expect a renewed debate over the value and necessity of the examination soon.)
–
LOSER: First-choice matching.
We won’t know for sure till the full NRMP report is released in May… but I’m betting we’ll see a record low for the proportion of graduating MDs who got their first choice in the Match.
This is hardly a hot take – I’m simply predicting the continuation of a consistent trend over the past 15 years.

Why is this happening? I say it’s Application Fever. The more applications students submit and programs receive, the more difficult it becomes for each to discern the other’s true intentions and interest. And I think this trend will continue – maybe with a little fluctuation from year to year – until we get the wherewithal to deal with Application Fever by implementing application caps.
–

WINNER: The Electronic Residency Application Service (ERAS).
Not only did the 2022 Match Week cap off the most voluminous – and lucrative – season of applications ever, it also marked the first year in recent memory in which ERAS did not crash or suffer major downtime during the SOAP.
According to their 2021 audit, the Association of American Medical Colleges took in revenue totaling $116,670,173 on ERAS – a 16% improvement from 2020 (which was itself a record-setting revenue total). The nicest thing that I can say about that is that at least some of that ransom – I mean, revenue – seems to have been invested in ensuring the system is function during the one week in which it’s essential that it do so.
–
WINNER: Preference signaling.
Following a successful pilot in otolaryngology, dermatology, internal medicine, and general surgery began using preference signaling for the 2021-2022 application cycle. (I covered the ups and downs of the ERAS preference signaling and secondary applications in a previous Mailbag.)
How well preference signaling worked out for the new specialties isn’t yet public (though I’m guessing papers are forthcoming). But the perception must be favorable, because many other specialties will begin using preference signaling and secondary applications next year.
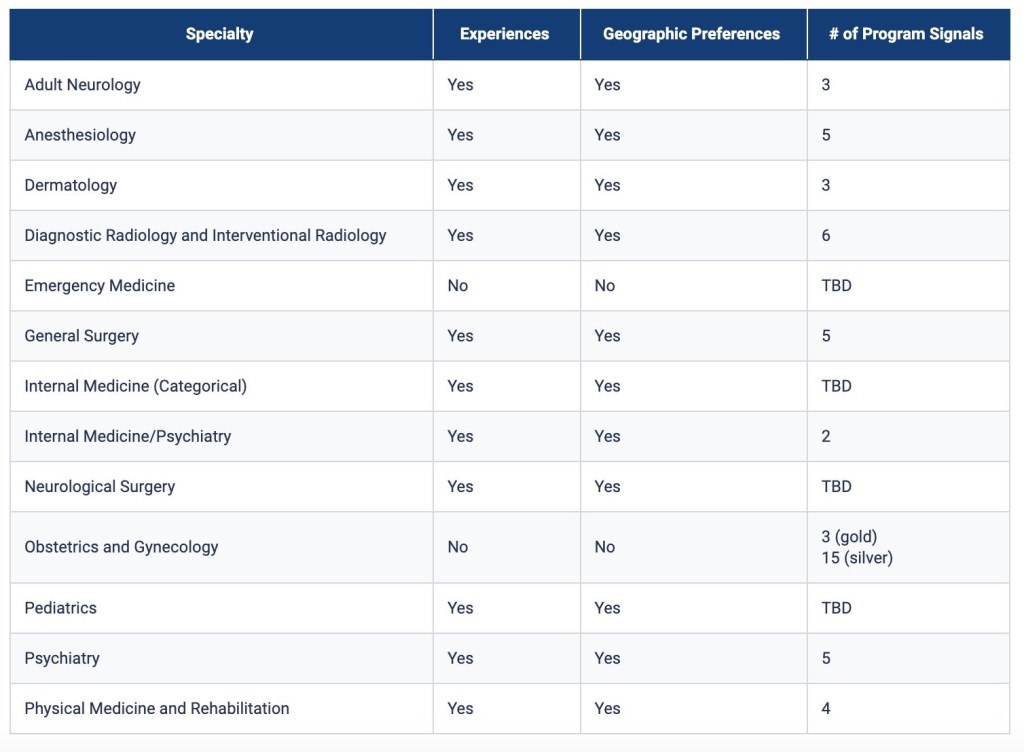
This is an important trend. The proliferation of preference signaling will lead to some unintended consequences that I’ll review in a future post. Moreover, the use of a tiered signaling system in OB-GYN is especially noteworthy and deserving of further analysis – so check back soon (or just subscribe already).
–
WINNER: Match Day celebrations.
After a couple of years of virtual Match Days, it was heartwarming to see old school, in person celebrations this year.
Look, COVID-19 is not going away. But watching fourth years open letters with their families and classmates makes it feel like – in some ways, at least – nature is healing.
–
WINNER: Match Week myths.
Hey, have you heard that we don’t have enough residency positions for all the students who graduate U.S. medical schools each year? Me, too!
Thing is, it isn’t true. Neither is the claim that the number of graduating U.S. medical students is growing more rapidly than the number of residency positions available.

In reality, there are around 1.33 PGY-1 positions available for each graduating U.S. MD and DO student. However, there are not enough residency positions for every single applicant when you include re-applicants and international medical graduates – then, the ratio of positions to applicants falls to 0.85. But as you can see from the red line on the graph above, the disparity between positions and applicants is not increasing – it’s been stable for the past 25 years, with ratios ranging from 0.75 to 0.88.
Still, myths about the paucity of residency positions take on new life each Match Week, when they get coupled to heartbreaking stories of unmatched applicants.
And this year, just like years past, there was no shortage of heartbreaking stories. All told, around 2000 U.S. MD and DO seniors went unmatched (along with over 5000 IMGs). Although many unmatched graduates find spots in the SOAP, many don’t. At best, having so many unmatched doctors is a horribly inefficient use of a precious resource.
The reason I bristle when I hear the myths quoted above is not because I don’t care about unmatched applicants. It’s because I do. Unfortunately, the false claim that there aren’t enough positions for the U.S. MDs and DOs makes it seem like the solution is simple: Just make more residency spots! Haven’t you heard there’s a DOCTOR SHORTAGE?!?
It’s not so simple. I mean, look around – we have more than enough residency positions for all U.S. MDs and DOs to match, yet many don’t. It’s not just a numbers game.
The reasons U.S. graduates go unmatched are varied, but one common one is that they weren’t interested in the positions that are available. For instance, we need more family physicians – but if you create more family medicine residency positions, I doubt you’ll see any more U.S. graduates matching into them. (Instead, there will be just as many going unmatched in orthopedics and otolaryngology and OB/GYN.)
Of course, if you increase the number of residency positions – even in specialties that are undesirable to graduating U.S. medical students – many other applicants will eagerly fill them.
In most ways, this is a great thing. We are very lucky that the United States is the preferred destination for some of the most talented IMGs. But it must be understood that the potential supply of residency applicants from around the world is inexhaustible. Ensuring that all IMGs match isn’t a sensible or realistic policy goal. No serious person can possibly believe that simply adding residency positions, year after year, until every single applicant has one is good for patients; doctors; the practice of medicine; or the American healthcare system writ large.
Real solutions are more nuanced. The goal of residency training is to provide a sufficient physician workforce to care for our population – so we absolutely should to expand residency positions to ensure we can do that. Even then, just having more doctors doesn’t guarantee patients get more access to care – there’s a distributional aspect to doctor shortages that we often ignore.
Lots of applicants would love to become dermatologists – but if we expand residency positions, we need some way to ensure we end up with more dermatologists who accept Medicaid or work in rural areas or care for medically-complex patients. (We can probably manage without more cash-only cosmetic dermatologists in Miami or Orange County.)
So we also need to provide right incentives for hospitals to create positions in the specialties we need, and for the doctors who fill those positions to then practice in the geographic locations where patients need them. There’s no magic solution, but there are are many policy efforts that could help. So if you want to be part of the solution, stop spreading misinformation and join in.
–
YOU MIGHT ALSO LIKE:
How Much Are Resident Physicians Worth?
Mailbag: ERAS secondary applications and preference signaling
Match Day 2021: Winners & Losers Edition
–
ADDENDUM (03/22/22) – I’ve gotten more than the usual amount of negative feedback about this post, especially related to my final points about unmatched physicians and the physician workforce. I feel like I need to clarify some things.
A couple of readers have suggested that arguing against a residency position for every applicant encourages an anti-equity “scarcity mindset” when instead we should take an “abundance mindset” and grow the pie enough for everyone to have a piece.
The sentiment that underlies this argument resonates with me – but folks, as a policy initiative, it is just not realistic.
This year, there were 8474 unmatched applicants. There were 36,277 PGY-1 positions offered in the Match. So suppose I wave a magic wand, and I give a residency position to every single unmatched applicant. Assume for the moment that all of the new positions are financially solvent and educationally rigorous. What happens next year?
I’ll tell you what will happen – more applicants will apply for the now 44,751 residency positions available. Remember, many capable and qualified IMGs choose to not to go through the expense and personal sacrifice of pursuing residency training in the United States simply because of the long odds. But if we guaranteed a residency position to all comers, more applicants will come – so we’ll need to expand residency positions again.
Soon, new medical schools will pop up. Right now, not every bright student who wants to get into medical school gets in – so any new school, U.S. or overseas, can tap into a ready stream of applicants. The school’s educational quality or tuition costs won’t matter much since their graduates are guaranteed to get a residency position if they only apply.
After a few years of this, we’ll have to manage the torrent of new doctors finishing residency. I don’t think that’s going to go very well, either. Sure, we’ll fix the doctor shortage – but if you continue to add residency positions every time an applicant goes unmatched, cycle after cycle, it won’t take long to have legions of unnecessary doctors trying to make work for themselves in whatever way they can. No one – and I mean, no one – benefits then.
Several readers believed that my focus on U.S. MDs and DOs was similarly unfair and inequitable. I will probably not be able to convince these readers otherwise, but it’s important for everyone in this debate to understand that American medical schools receive enormous financial support from the government. This extends well beyond direct funds from the Department of Education or handed out to state schools through their state legislature, and includes tax exemptions/breaks as well as access to government-backed student loans.
The uncomfortable reality is that it is politically untenable for there ever to be a circumstance in which U.S. graduates matched at lower rates than graduates from schools overseas. It’s one thing for taxpayers to support medical schools if those schools produce physicians that care for the citizens – but it’s another thing if those schools graduate doctors that can’t contribute to the workforce and default on their student loans. If such a circumstance ever did come to pass, it would inspire a vigorous response from politicians, who would likely create an explicitly-tiered system rather than the – admittedly unfair – implicit one we have now.
Another reader pointed out that some IMGs are fleeing unstable political environments or conflict zones, and that securing a residency position can mean the difference between life and death for that doctor and their family. I don’t doubt for a second that this is true. I would only counter that, if you care about helping people in these countries, expanding residency positions is a horribly inefficient way of doing so.
Residency training has to be regarded as a process to generate physicians that will serve patients – not as a means of social welfare. The number and distribution of residency positions can only properly be based on a careful assessment of the number of doctors that our patients need in the future – not the number of applicants for those positions now.
(And for the record, I do believe that residency positions should be expanded – with the caveat that increased GME funding or expanded positions be coupled to other incentives to ensure that the expansion actually results in more physicians serving the patients that need them, as I suggested above.)
As always, though – keep those comments coming. I learn lots from my readers, even when we disagree.
