Last week, the Association of American Medical Colleges’ Electronic Residency Application Service (ERAS) announced some changes for this year’s residency applicants in three specialties (internal medicine, dermatology, and general surgery).

This led to a surge of DMs and e-mails into my inbox, and necessitated this latest mailbag to clear them out.
As always, these are real questions from real readers – but distilled down for clarity and anonymity.
–
Have you heard that ERAS is now requiring applicants in certain specialties to provide “an indication of their top residency programs of interest”? Isn’t this a Match violation?
Yes, I have. And no, it’s not.
It’s true, the NRMP’s Match Participation Agreement (MPA) forbids programs from soliciting “verbal or written statements implying commitment.” But that’s not what this is.
Instead, it’s just a formalized way of expressing interest in a program – which is expressly allowed under the MPA. (Section 6.2 notes that “both applicants and programs may express their interest in each other.”)
Essentially, it’s the same voluntary preference signaling that otolaryngology used in the 2020-2021 Match cycle – only instead of the program directors’ association requesting the signals of interest from applicants and distributing them to programs, ERAS will do it instead.
–
Could you please explain why ERAS is making us identify our top programs this year? This seems very unfair. Don’t most applicants decide how to rank programs after they’ve met people (and learned information, good or bad) at their interview?
You’re right, the interview is the biggest determinant of rank order list position for programs and applicants alike. But unlike the rank order list, this initial list isn’t binding.
Viewed in the most favorable light, it’s a way for applicants to ensure that their application isn’t overlooked by a program where they have sincere interest. Viewed in a more realistic light, it’s a tool for programs to ensure they’re spending their time interviewing applicants who actually want to come to their program.
(If you’re interested, I wrote a Winners & Losers piece on preference signaling after otolaryngology announced their plan last year. I also argued the case against it at the NRMP meeting in the fall.)
–
The Match rate in ENT was brutal last year. So why is ERAS expanding preference signaling if it didn’t help otolaryngology? Why expand a failed experiment?
I wouldn’t call preference signaling a “failed experiment.” Actually, the preliminary data from otolaryngology’s experience have been released – and they look encouraging.
Some highlights:
- Most applicants (91%) chose to send signals
- All programs chose to receive signals
- 93% of applicants received at least one interview offer from a program to which they sent a signal; 61% received 3 or more interviews from their 5 signals
- The probability of receiving an interview offer was 58% at a signaled program vs. 14% for a non-signaled program
- Over 70% of applicants agreed that they were satisfied with signaling
But yeah, if your measure of success is the Match rate, preference signaling isn’t gonna help you. The only way to get more applicants to Match is to add more positions.
This is a key point: the Match is, in many ways, a zero sum game. Require supplemental applications or don’t, allow preference signaling or not – the point is, you can’t make everyone win. Not everyone can go home happy on Match Day – and one applicant’s win is almost necessarily another’s loss. The best we can do is make sure that the competition is fair.
So is it?
–
General surgery applicant here. I’ve worked extremely hard to become a competitive applicant (top 20 MD school, USMLE Step 1 25x, Step 2 CK 27x, several research publications) and I never considered that I wouldn’t match until ERAS came out with this garbage today. Why should I have to indicate my interest in a program before they indicate their interest in me? What happens if I indicate interest to the wrong programs and my backups pass over my application because otherwise inferior applicants indicated their interest? I hope you will use your platform to advocate against this unnecessary and unfair system.
Hold that thought for a second…
–
I’m a DO applying in general surgery for Match 2022, and it seems like this proposal is going to screw over applicants like me. It feels like I’m being forced to tip my hand and show my cards before programs have to show theirs. Now, if I don’t send a signal my application will be passed over. I don’t see how this benefits applicants other than Ivy Leaguers, while applicants like me have to overcome an already biased and unfair system that now will become even more so.
Okay, I hear you, but lemme just check one more e-mail…
–
What do you think of the requirement that general surgery applicants have to indicate their top programs of interest? I think there will be a lot more unmatched applicants from state medical schools (like me). The top tier applicants will use their signals to get in at the top programs, while international graduates and lower tier applicants will now Match because of the signal. It will systematically disadvantage strong but not elite applicants while advantaging those at the top and bottom of the scale.
Hmm… so if top-tier, medium-tier, and “lower-tier” applicants all think a system is unfair, does that actually mean it’s fair?
After considering it carefully, I don’t think that preference signaling systematically advantages or disadvantages any particular group. But it will systematically advantage those who send their signals wisely – and punish those who do not.
–
How should residency applicants use their signals? Should I shoot my shot at the top programs, or save some for mid-tier programs, too? Is it worth sending a signal to my home program even if they always interview internal applicants?
To answer this question, you first have to understand how programs are likely to use the signals of interest.
Programs are likely to use signals of interest in their initial applicant screening (i.e., in deciding whom to interview) rather than when they are creating their rank order list.
From an applicant’s standpoint, then, the value of a signal is in increasing the probability of an interview at a program to which the applicant might not otherwise have received an interview.
If you signal a program where you know you’re unqualified and have a 0% chance of being offered an interview, sending a signal probably isn’t gonna change that. On the other hand, sending a signal to a program that was already going to give you an interview wastes a signal and doesn’t leave you with anything more than you would have had without sending a signal. (Otolaryngology explicitly asked applicants to not send signals to their home program or programs where they did an away rotation for this very reason.)
In other words, an applicant should send signals of interest to programs where they have a non-zero, but less than certain, probability of receiving an interview – provided that they actually have real interest in attending those programs. If you use your signals to get your foot in the door at programs you don’t really want to attend, you just played yourself.
Applicants should also consider that the value of a signal is likely to vary from one program to another. The more signals a program receives, the less meaningful each becomes. And the number of signals a program receives varies widely.
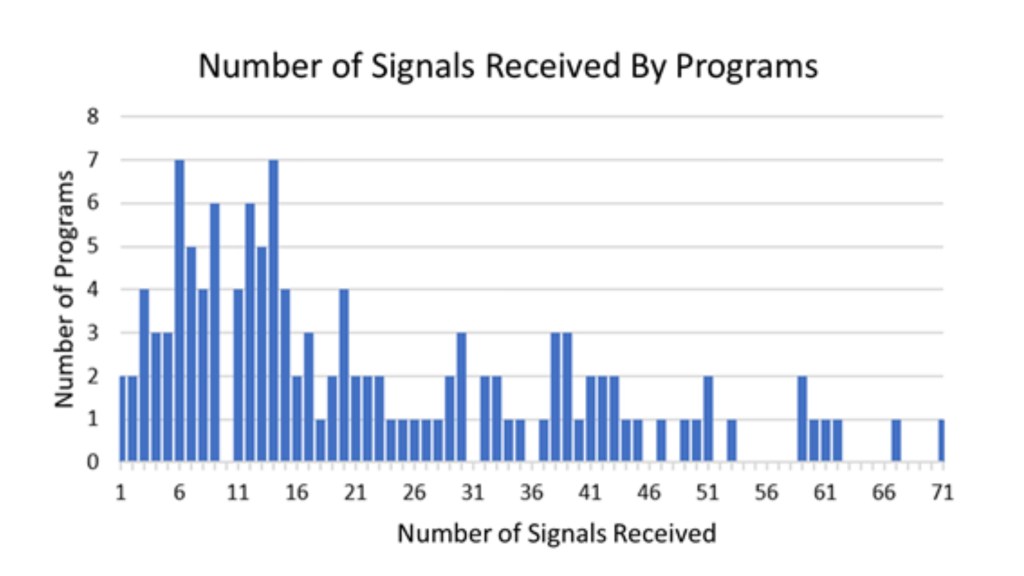
In last year’s otolaryngology Match, the top 10 programs received 21% of all signals submitted; the top 20, 38%; and the top 30, 52%.
The bottom line:
If I were applying in dermatology, IM, or surgery this year, here’s how I’d decide how to send my signals.
First, I’d carefully research programs and come up with a list of the top 10 places where I’d honest-to-God hope to spend my residency.
From that list, I’d eliminate any at which I thought I had a <10% or >90% probability of receiving an interview.
If the remaining list was longer than the number of signals I have to spend (and so far, these specialties have not announced what that number will be), I’d break the tie by prioritizing programs where I had more heartfelt interest and/or the program seemed likely to receive fewer signals (meaning my signal would likely matter more).
–
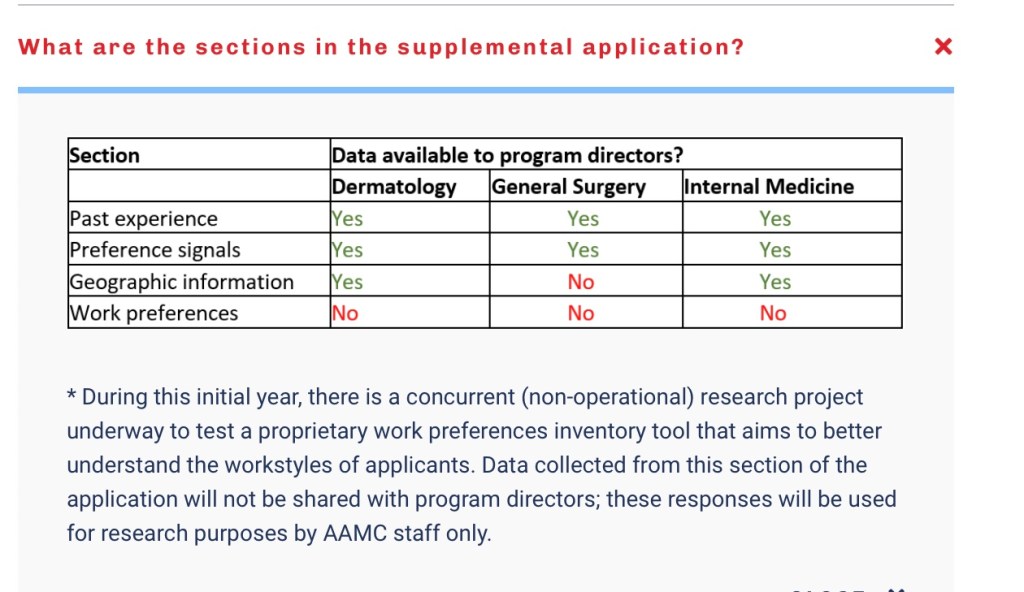
What’s the deal with this “research” that the AAMC are conducting on the secondary applications? Can applicants opt out of it?
Beats me. I haven’t heard any information beyond the description above.
My guess is that the AAMC’s “proprietary work preferences inventory tool” would be something that they would sell or market to programs in the future to help programs find applicants who share the program’s “workstyle.” (If so, I don’t think their tool will ultimately provide much useful information: as soon as applicants perceive that programs are searching for a particular “workstyle,” they’ll answer the questions indicating that that’s their workstyle, too.)
I also don’t know if ERAS will allow an official opt-out of their research (though ethics and common decency would argue that they should). I seriously doubt they will compel applicants to provide answers, and I’m absolutely certain they can’t compel honest ones. So if I were an applicant, I wouldn’t stress about this part too much.
–
I’ve seen you write about “Application Fever” and how program directors are overburdened with applications. So I don’t understand this latest announcement from ERAS about secondary applications. Why would program directors want MORE information to review?
Ah, but it’s exactly because of Application Fever that certain specialties have requested this.
You’re right – there’s a ton of information in ERAS. But ERAS is also such a clunky system that much of that information is difficult to efficiently access.
The idea behind some of these secondaries is to put key information front and center, allowing program directors to more efficiently and effectively evaluate applications without using a single quantitative metric (like a USMLE score).
–
I thought I was done with secondary applications when I got into med school. Apparently not. I spent around $1000 on secondary applications four years ago and I’m still bitter about it. I realize that ERAS says there’s no extra cost for these secondaries, but do you think that is going to change in future cycles? Is this just another way for them to make money?
It is a way for them to make money… but I actually do think the secondaries will remain free. Let me explain.
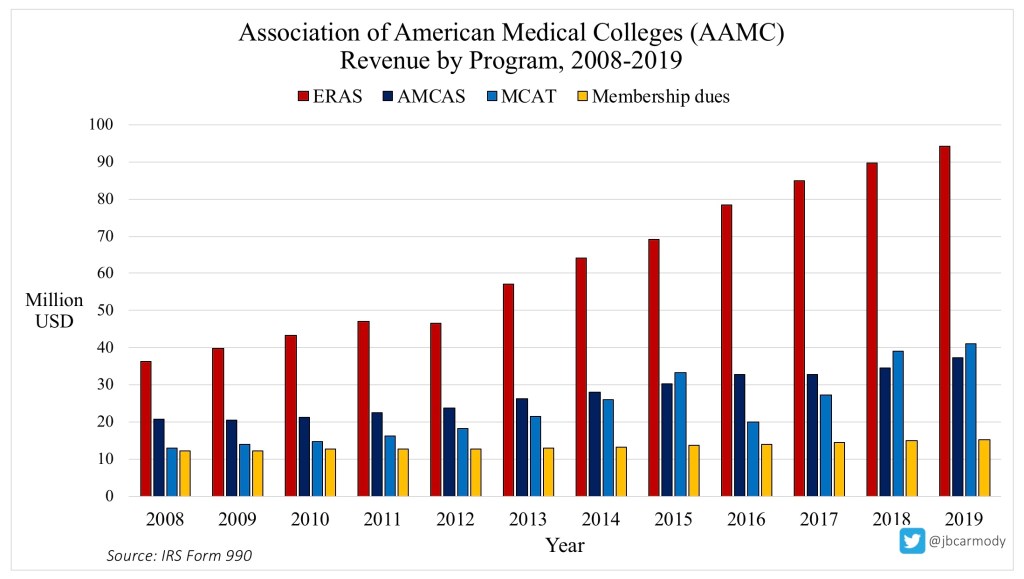
ERAS is the AAMC’s cash cow. It brought in $94 million in revenue in 2019, and as you can see from the graphic above, revenue growth from ERAS has dramatically outpaced growth in the AAMC’s other programs.
What’s fueling this growth? Application Fever.
As applicants submit more and more applications each year, they line the AAMC’s coffers more. Of course, this overapplication puts more pressure on programs, and leads reasonable people to ask: why not implement application caps?
Application caps would severely constrain the AAMC’s revenue growth. And they’re willing to jump through some hoops in order to keep people from thinking about them too much.
To me, that’s what all of this is. Preference signaling and secondary applications grease the wheels of the system just enough to keep it going. They enable continued overapplication by giving program directors the tools they need to ignore a certain amount of it.
Look, I’m not opposed to simple secondaries or preference signaling. (I was honestly a little surprised by how many people contacted me expressing concern that these systems were unfair.)
But we’ve got to be honest that neither secondary applications nor preference signaling gets at the root of our current troubles. Ultimately, it just creates a new layer of strategy for applicants to ensure their own success in a zero-sum game. It creates just enough efficiency for programs to keep their focus off overapplication – and leave the AAMC’s hand in applicants’ pockets.
You know what they say: the more things change…
–
YOU MIGHT ALSO LIKE:
The Case for Residency Application Caps
