
Today, the Coalition for Physician Accountability – the alphabet soup of organizations overseeing medical education and physician practice in the United States – issued an important statement. Among other things – such as strongly discouraging away rotations and delaying the ERAS opening until October 21 – it recommended that all interviews for the upcoming residency application season be conducted virtually.
This was not a surprising move. I discussed it a few days ago on Twitter. But just for fun, let’s break it down one more time.
Who wins – and who loses – when interviews go virtual?
–
WINNER: Homegrown applicants.
Every year, many students choose to stay for residency at the same institution at which they attending medical school. In fact, in some competitive specialties, 21% of positions are filled by these internal candidates. This year, without the ability to vet other applicants in person, program directors may gravitate toward homegrown applicants even more.
–
LOSER: DOs and IMGs.
Staying at your home program is a good choice… if you have a home program. International medical graduates (IMGs) don’t – and some applicants from osteopathic medical schools may not have an affiliated hospital with a residency program in their desired specialty, either.
(Combine this with the elimination of most away rotations, and DO/IMG applicants to competitive specialties may be facing even more of an uphill battle.)
–
WINNER: Student travel budgets.
Previously, many applicants spent upwards of five figures on their interview tour. You gotta really treat yo self to spend that much doing Zoom and WebEx interviews in your living room.
–
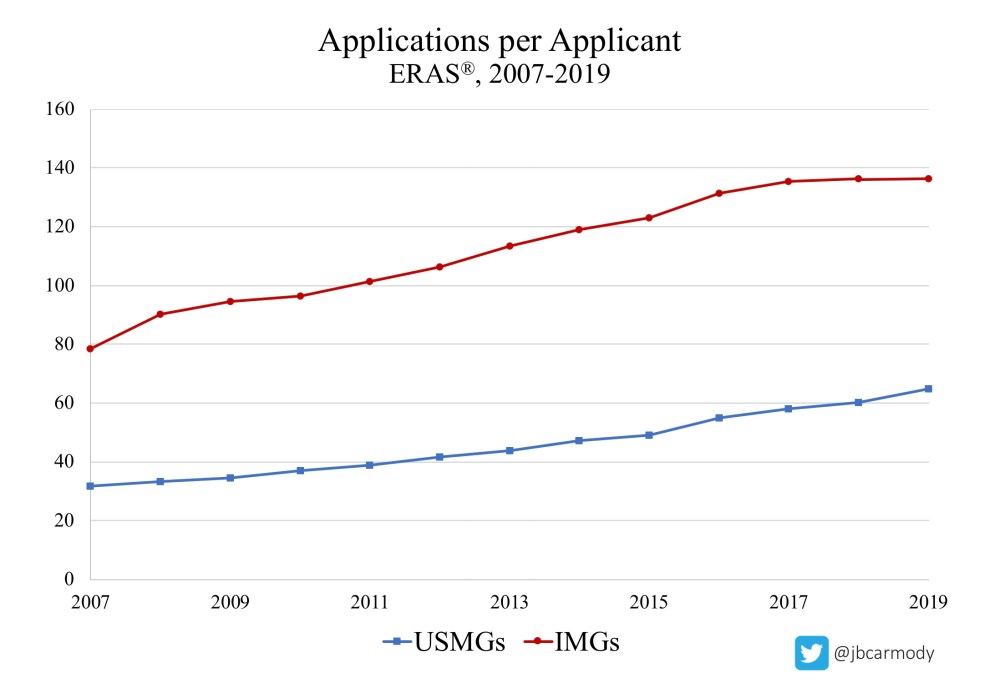
LOSER: Student ERAS budgets.
The number of applications students submit has been rising steadily for years. And even before this announcement, the 2020-2021 application cycle was shaping up to be a wild one, with students facing genuine uncertainty about how their applications will be evaluated. Throw in virtual interviews on top of that, and things will be even more unpredictable. Will students respond to that uncertainty by applying to even more programs? My guess is yes.
_
WINNER: The AAMC.
When students apply to more programs, no one benefits more than the Association of American Medical Colleges, corporate sponsor of the Electronic Residency Application Service (ERAS).
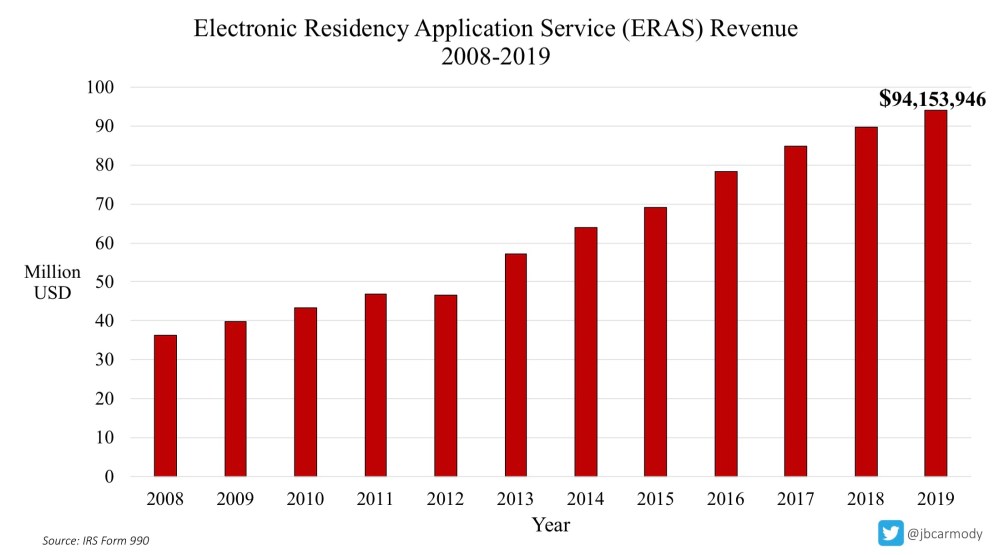
Last year, ERA$ generated $94,153,946 in revenue for the AAMC. If students apply to more programs, look for their coffers to swell even further.
–
LOSER: Community and lesser-known programs.
Quick quiz: Which program would YOU be more willing to rank #1, sight unseen?
A) a lesser-known or community program
B) whichever program Doximity or U.S. News & World Report says is the “best” program
(Yeah, me too.)
–
WINNER: Programs with good websites, videographers, and authentic social media presence.
If you want applicants to feel comfortable ranking your program without ever setting foot on the grounds, then you’ve gotta give them as much information as possible. Programs that invest in building an informative website; who make high-quality video tours; or who have resident-run Instagram or Twitter accounts will have the inside track when students make their rank order lists.
–

LOSER: Programs that don’t interview more applicants.
Back in the old days, when applicants had to interview in person, there was sort of a natural cap on the number of interviews an applicant could attend. Apply to 50 programs if you want – but you’ll run out of time, money, or both before you can pull off that many interviews.
Virtual interviews don’t provide these same bounds. This season, it may be very possible for a well-qualified but nervous applicant to do 50 interviews from the comfort of their own home.
The problem is, most programs have worked out their formula for how many applicants they need to invite, interview, and rank in order to fill. Those calculations are going to get skewed if well-qualified applicants choose to interview at more programs.
Take, for instance, a typical otolaryngology or family medicine program in which 25% of invited applicants historically choose not to interview. If those applicants now decide to interview – “just in case” – then they may squeeze out spots for other applicants who were more likely to rank the program highly. Unless programs interview more applicants – or better yet, we impose an interview cap – we may see an increase in both the number of unmatched applicants and unfilled programs.
–
WINNERS: The MSPE and personal statement.
According to the NRMP’s Program Director Survey, interpersonal skills and interactions with faculty and residents during the interview/visit are the most important factors when ranking applicants. Will virtual interviews carry as much weight as in-person interviews when applicants are ranked? Probably not.
Of course, with many applicants unable to obtain USMLE scores, complete away rotations, or even work closely with faculty to get letters of recommendation, what will fill the void? The Medical Student Performance Evaluation (MSPE) will probably gain more importance – which makes it even more critical for programs to demand that the dean’s letter be meaningful. Even the often-unread and typically-formulaic personal statement could actually factor into recruitment decisions this year.
_
LOSER: Bad reputation cities.
Generally speaking, it’s easier to get young professionals excited about moving to Seattle or Denver than it is to get them fired up about living in Cleveland or Baltimore. But many applicants who actually visit these ‘bad reputation’ cities end up discovering that they aren’t so bad after all. (Of course, if you have to make decisions based on what you can see on Google Maps, where would you go?)
_
WINNER: Malignant programs.
Even the most rotten and soul-crushing program can probably turn on enough charm to survive the scrutiny of what amounts to a FaceTime call. For many applicants, the most telling interactions occur during the visit, but outside the formal interview. Maybe it’s the attendings you see snapping at each other on rounds. Or the intern you stumble upon crying in the stairwell during the hospital tour. Or the dead-eyed residents falling asleep at the pre-interview dinner. The point is, virtual interviews make it a lot easier to sweep this kind of dirt under the rug.
(On the other hand, programs that already have a bad reputation will have a tough time living it down this year. Word of mouth is gonna matter a lot more – so those that have already been named and shamed may spend another year in purgatory.)
–
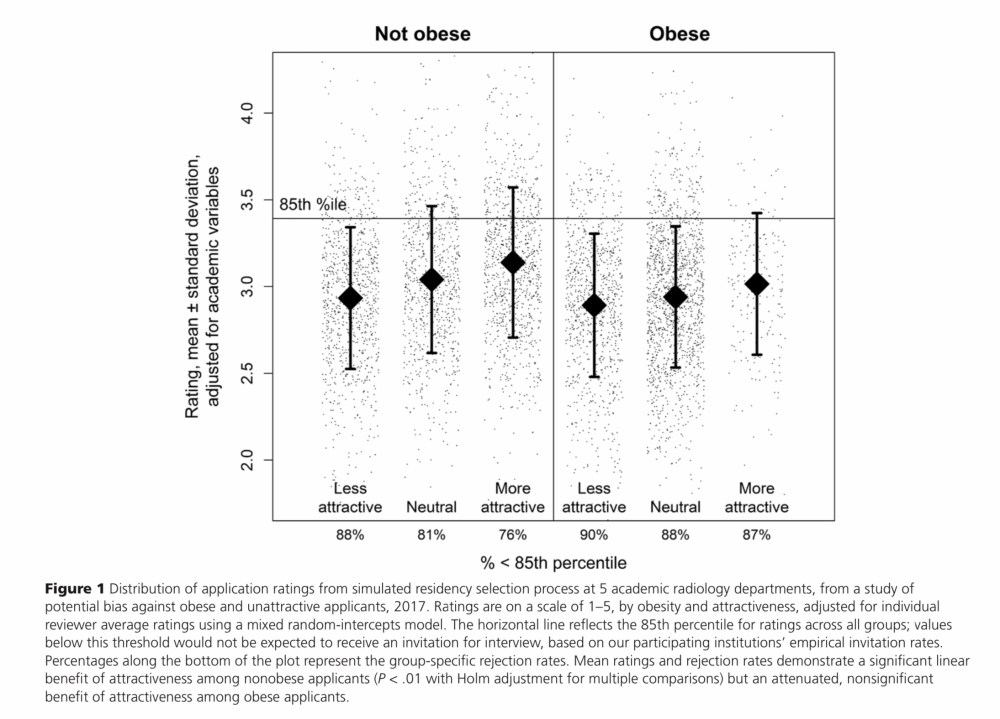
Maxfield CM, et al. Acad Med 2019; 94(11): 1774-1780. PubMed.
WINNER: The attractive and non-obese.
Already, these applicants enjoy an advantage: being facially attractive is equivalent to around a 10-point increase on USMLE Step 1, while being non-obese is similar to having 2 additional research publications. These effects will only be magnified if all PDs have to go on is somebody’s head on a screen.
–
LOSER: Women and under-represented minorities.
Will superficial virtual interviews be more influenced by implicit bias than than more in-depth real ones? I hope I’m wrong – but my guess is yes.
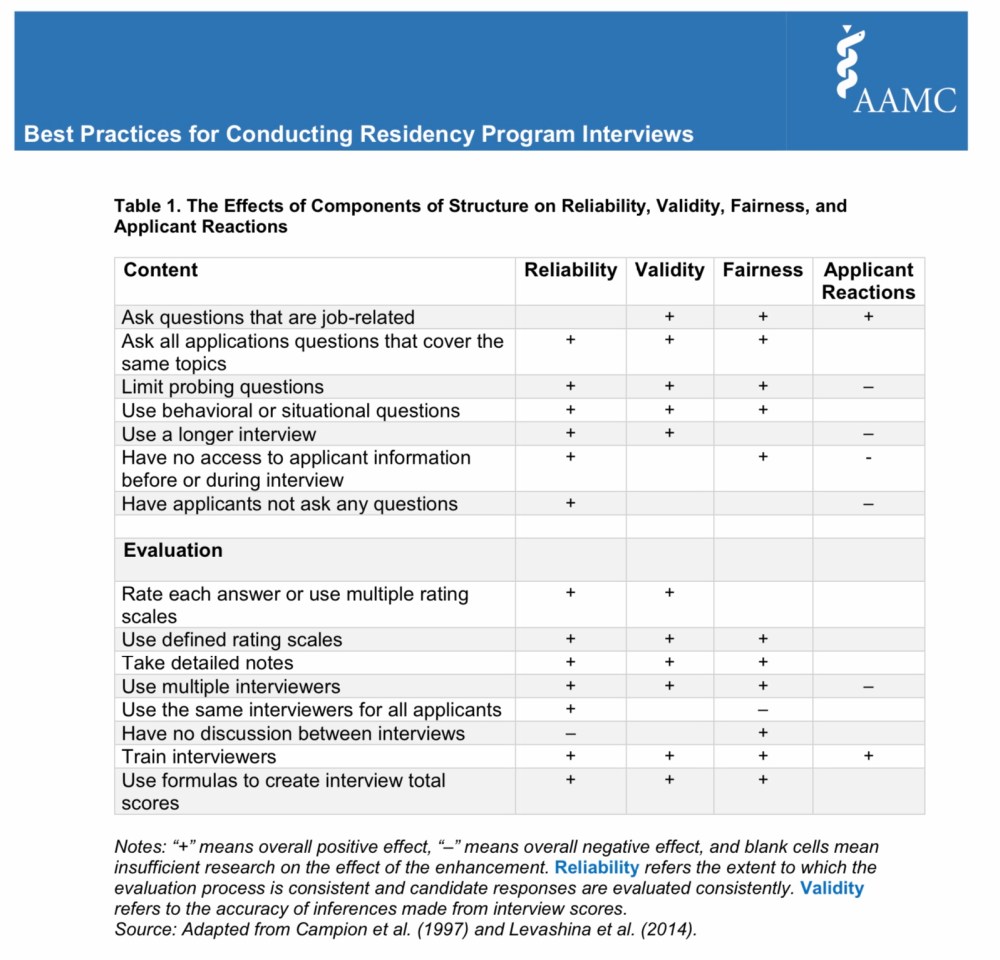
From the AAMC’s Best Practices for Conducting Residency Program Interviews.
(Of course, more bias is not inevitable. In fact, COVID-19 provides an opportunity for residency programs to revamp their unstructured interviews, reduce bias, improve validity and reliability, and leave a better system in their wake.)
–
WINNER: Zoom backgrounds and high-speed Wi-Fi.
All else being equal, the applicant whose virtual interview is professional and without technical interruptions is going to win out over the guy sitting in his apartment kitchen wearing boxers and having to get up to let the dog out in the middle of his interview. Students should plan accordingly. (Better yet, every medical school’s Office of Student Affairs could go ahead and invest in a few microphones, HD cameras, and ring lights, and create a small studio where students can conduct their interviews.)
–

On May 8, the USMLE announced that they were exploring a new, virtual format for the Step 2 CS exam.
WINNER: Students who take the new and improved USMLE Step 2 CS.
Interviewing in a new format may catch some students off guard. But not the lucky students who get to take the new and improved virtual USMLE Step 2 CS! These students will come to interview season ready to rock and roll, having proven that they have the chops to succeed in the modern, fast-paced virtual healthcare environment.
(Okay, I’m sorry. I just couldn’t help myself. The new Step 2 C$ exam won’t benefit any students, and the whole premise sounds like it was drawn up on a cocktail napkin at the Pyramid Club. Expect more comment from me soon.)
–
LOSER: The Class of 2021.
Yeah, again.
The same class whose clerkships were cut short; whose away rotations and Step 2 CK test dates were cancelled; who get to be guinea pigs for the new Step 2 C$ exam (still for the low, low price of $1300!) is getting hit again.
(And yes, the medical school Class of 2020 had a rough go, too, losing their Match Day and graduation celebrations to COVID-19. But I’m gonna be honest, I don’t think the prospect of the Class of 2021 getting to have those things is looking too good, either.)
–
WINNER: Public health.
I have deep reservations about this policy and what it will mean for both applicants and programs. But ultimately, we’re all in the business of helping patients – and the concept of 40,000 people flying all across the country from one COVID-19 hotspot to another is just untenable.
–
It’s going to be a recruitment season unlike any other – and there will be bumps in the road, for sure. But uncomfortable as it may be, this move also provides opportunities for reforms that will be beneficial even when in person interviews return. Whether we seize them is up to us.
