
I.
In March 2020 – just as life in the United States was coming apart due to COVID-19 – a company named M&B Multi-Services found itself in a fortunate business position.
At a time when hand sanitizer was a precious commodity, M&B happened to have a few boxes of Purell on hand.
Usually, they sold these 8 oz bottles sold for around $7 – but that was before COVID-19. Sensing an opportunity to profit, they sold their remaining stock for up to $75 per bottle.
In so doing, they broke the law.
Like many other states, Pennsylvania has a price gouging statute. The law makes it illegal for business to increase prices for consumer goods by more than 20% during a state of emergency.
Because the Governor of Pennsylvania signed a disaster declaration on March 6, 2020 – and because M&B increased the prices on their Purell by significantly more than 20% – M&B ran afoul of the price gouging law. And so, last week, the Pennsylvania Attorney General sued M&B for over $1 million in damages.
We won’t tolerate illegal price gouging during this emergency, and we’re taking action every day to stop it.
–Josh Shapiro, Pennsylvania Attorney General
–
II.
The Educational Commission for Foreign Medical Graduates (ECFMG) is a 501(c)(3) non-profit organization founded in 1956 to assist international medical graduates (IMGs) seeking residency training in the United States.
The ECFMG often likens its role to that performed by the dean’s office at a U.S. medical school. It’s an apt analogy. The ECFMG’s primary purpose is to verify credentials and vouch for the professional readiness of IMGs to enter residency training. In fact, any IMG who wants to train at an accredited residency program in the U.S., must be ECFMG certified.
Put simply, the ECFMG has a monopoly on all the services related to IMGs entering the U.S. And lately, business has been very good for the ECFMG.
Over the past decade, their revenues have nearly doubled to ~$80 million per year, and by 2017, the ECFMG had amassed total assets valued at $197.8 million dollars. 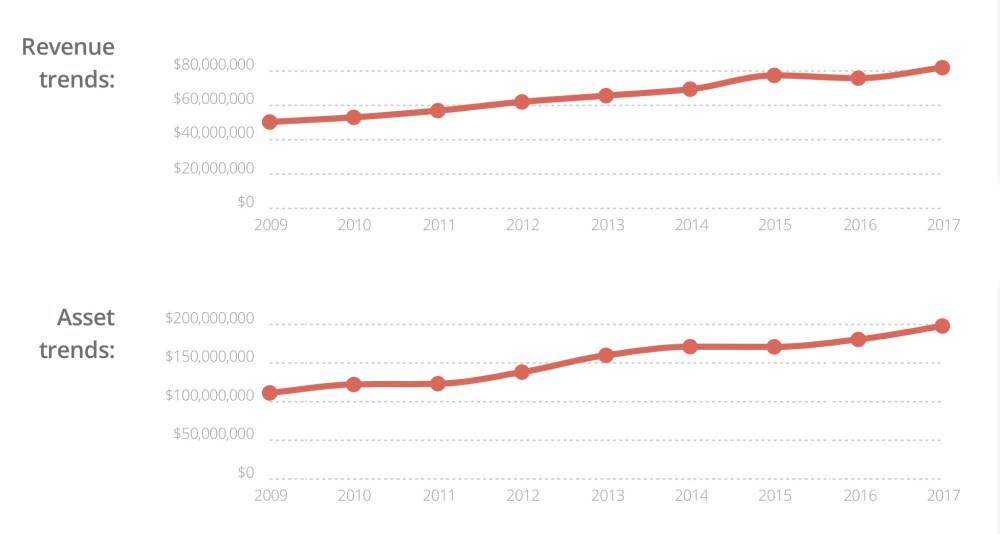
Financial trends for the ECFMG, from CauseIQ.
–
III.
At the same time that consumers were snapping up $75 bottles of Purell, the ECFMG was entering crisis mode.
The COVID-19 pandemic had made it impossible to safely administer the United States Medical Licensing Examination (USMLE) Step 2 Clinical Skills exam. From a business standpoint, this was a catastrophe.
Most of the ECFMG’s revenue is derived from administering the USMLE to IMGs. With a price tag of $1600, the Step 2 CS exam is the most expensive test in the series, and the ECFMG is a joint stakeholder in the Clinical Skills Evaluation Collaboration, which runs the five Step 2 CS testing centers in the United States.
But now, those testing centers were going to sit fallow for at least 12-18 months while the USMLE sought to “revitalize” clinical skills assessment.
And there was another problem, too. Without the Step 2 CS exam, the ECFMG had to figure out how they would certify new residency applicants.
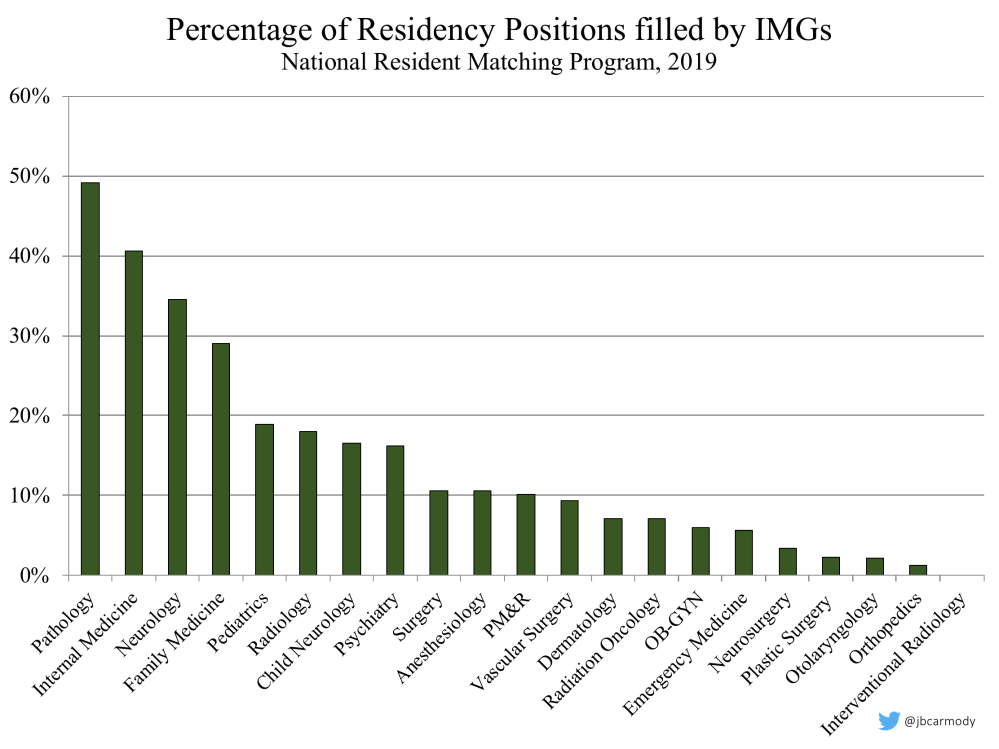
IMGs fill around 20% of all residency positions each year – and significantly more in certain specialties.
Historically, the ECFMG had required the Step 2 CS exam in order to confirm that IMGs possessed adequate spoken English proficiency and sufficient basic clinical skills to succeed in U.S. graduate medical education programs. What would they do without it?
It was too late to try to make a new test. They needed a workaround.
–
IV.
For U.S. medical schools – many of which required Step 2 CS as a graduation requirement – the workaround was easy to find. They’d just pretend Step 2 CS didn’t exist. Their students would be allowed to graduate and participate in the Match, provided that they met the school’s other academic requirements.
And despite all of the high-minded talk in the old Step 2 CS debates about how the public demands a clinical skills examination, and that the CS exam was essential to maintaining public faith in physicians, and that patients would never trust doctors who hadn’t passed CS, the public outcry to this decision was entirely inaudible.
Even the Federation of State Medical Boards – which had previously required passing Step 2 CS to register for the penultimate Step 3 exam – agreed to play along. U.S. graduates would just proceed through training and licensure as if there had never been such a thing as the CS exam.
Practically-speaking, this was possible because the overwhelming majority of U.S. medical students pass the Step 2 CS exam. But not all do. During COVID-19, medical schools, residency programs, and even state licensing authorities all agreed to tolerate the ~5% chance of graduating, matching, or licensing a physician who would not have passed Step 2 CS on their initial attempt.
If everyone was willing to accept this ~5% risk for U.S. medical graduates – why not for IMGs as well?
–
V.
The term “IMG” applies to a wide array of physicians. Around one-third are U.S. citizens. Some have extensive practice experience; others are freshly-minted graduates. Some trained in countries whose healthcare resources are very limited, others in wealthy nations with modern hospitals as advanced as our own. Many are native English speakers; others have to translate their medical knowledge into a new language.
Taking all comers, only 73% IMGs passed the CS exam in 2018. But with a little work, the ECFMG realized that they could carve out specific groups of IMGs who statistically would be expected to have a similar CS pass rate as U.S. students.
We believe the people who qualify through these pathways will be as qualified as anybody who’s come through in the past.
–William W. Pinsky, MD, ECFMG CEO
First, they limited access to applicants with stronger performance on earlier sections of the USMLE (by excluding applicants who failed Step 1 or Step 2 CK more than once).
Next, they reduced the pool of potential applicants to those who could pass the Occupational English Test.
And then, to further limit certification to only the groups with the highest pre-test probabilities of passing Step 2 CS, applicants were required to satisfy the criteria in one of five new pathways:
- Physicians already licensed to practice medicine in another country
- Applicants who already passed a clinical skills exam similar to USMLE Step 2 CS (such as those offered in the U.K., Ireland, Canada, New Zealand, Australia, Switzerland, or Chile)
- Applicants from certain accredited schools (those accredited by an agency recognized by the World Federation of Medical Education)
- Applicants from medical schools who participate in the U.S. Federal Student Loan Program (a group of around 20 schools that enroll a significant number of U.S. citizens, including the “Big Four” Caribbean medical schools: Ross, St. George’s, American University of the Caribbean, and Saba)
- Applicants from schools who issue degrees jointly with a U.S. medical school (i.e., Duke University – National University of Singapore or Weill-Cornell Medicine – Qatar)
While some lobbied for the ECFMG to make the pathways more inclusive – in particular, to allow a pathway (other than pathway #1) to permit applicants from India and Pakistan, the two countries that supply the most residents to the U.S. – the ECFMG held firm to their original plan.
The only thing that had to be worked out was the nuts and bolts.
–
VI.
Last week, the ECFMG announced the specifics for its pathways, clarifying the deadlines and types of documentation needed.
They also announced the price: $900.
How was this fee determined? Beats me.
Thus far, I’ve been unable to find any public articulation of the ECFMG’s policy for determining any their fees. Their website includes a laundry list of prices and services, but is silent on how the prices are set. (They do helpfully note that all of the posted prices “are subject to change without notice.”)
For the record, I have reached out several times to the ECFMG for comment. They declined to respond altogether until after I called them out on Twitter. Since then, their only substantive response to me was that they “are working on preparing additional information on this topic and will publish it to the [ECFMG] website soon.”
(As an aside: When your organization refuses to provide its policy on how it sets fees, it tells me one of two things. Either no policy exists, and you just make it up as you go along, or releasing the policy publicly would make the organization look worse than stonewalling a good faith inquiry. Neither one is good – and so I started looking into the ECFMG’s finances a bit more. If you’re interested in what I found, come back soon for Part II. But for now, let’s get back to the $900 pathway fees.)
Could such a fee be justified?
I mean, there is some administrative effort required to verify an applicant’s medical license (Pathway 1) or test transcript (Pathway 2). But is there really $900 worth?
Interestingly, the ECFMG’s Electronic Portfolio of International Credentials (EPIC) used to provide credential verification for just $90 per credential – one-tenth the current going rate.
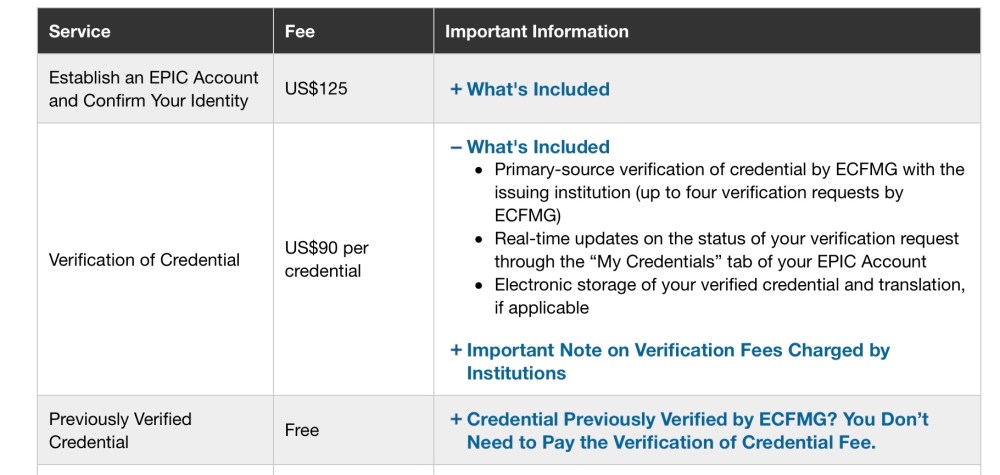
The markup for credential verification is similar to the markup on a bottle of Purell at the height of the COVID-19 pandemic.
From the screenshot above, note also that previously-verified credentials were free. This is a relevant because IMGs already had their basic credentials – such as their current enrollment in a bona fide medical school – verified as a requirement to register for the USMLE Step 1 and Step 2 CK exams.
So why are applicants in Pathways 3, 4, and 5 – who can pursue certification by virtue of the school they attended – also being charged a $900 fee? Is it really such a laborious and expensive task to look at a list of approved of medical schools and see if the applicant’s already-verified school of attendance is on the list?
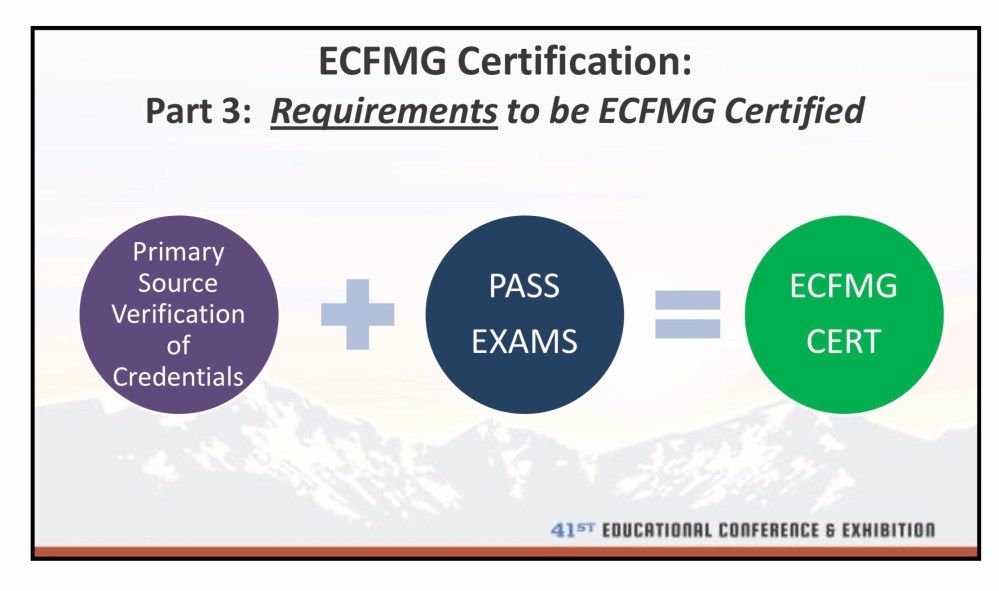
Slide from a 2017 presentation, given by an ECFMG vice president.
Historically, as shown on the slide above, ECFMG certification has required two things: credential verification and passing the USMLE. Those two requirements were also the sources of the ECFMG’s financial revenue.
And interestingly, as soon as the ECFMG started taking in less money on exams, the cost of verifying credentials went through the roof.
At best, it’s rent seeking. At worst, it’s price gouging.
–
VII.
The ECFMG is headquarted in Pennsylvania – the same state where the Attorney General is pursuing M&B Multi-Services for overcharging consumers on hand sanitizer.
Might the ECFMG be in violation of Pennsylvania’s anti-price gouging law?
Unfortunately, no.
The law applies to “consumer goods or services,” which are statutorily defined as as “those items used, bought, or rendered primarily for personal, family, or household purposes.” Certification needed to pursue medical training doesn’t apply.
And while the ECFMG may not have violated the letter of the law, I’d like to indict them for violating its spirit – and the general moral premise that underlies it.
The reason Pennsylvania – and many other states – have price gouging laws is to enforce a standard that should be just common human decency. You don’t use a crisis as a way to line your pockets.
The ECFMG serves an essential role. But they’re also, in the very literal meaning of hte term, a coercive monopoly. This gives them incredible power, and with it, an obligation to conduct their business fairly and transparently.
Any non-profit in such a privileged position should be able to articulate the calculations that went into the prices they set. Stonewalling is a bad look. So is increasing the cost of a required service ten-fold without any accompanying justification.
And if we’re offended by those who price gouge on Purell, shouldn’t we be just as aggrieved by those who profiteer on pathways?
–
ADDENDUM (08/28/2020) – Several hours after I posted this piece, I did receive – as promised – an e-mail directing me to the ECFMG’s statement on this issue.
–
YOU MIGHT ALSO LIKE:
ECFMG Finances, Part II: By the Numbers
Step 2 CS, Part One: How Did We Get Here?
