In early October 2020, President Donald Trump was admitted to Walter Reed Medical Center with COVID-19. Soon, curiosity swirled around his attending physician: Sean Conley, DO.
On social media, some ill-informed observers challenged Dr. Conley’s credentials, questioning whether a DO was a “real doctor” and had the requisite skills to treat the President of the United States of America.
Soon, the internet lit up as medical professionals from all backgrounds explained that yes, MDs and DOs are equivalent.

The American Osteopathic Association clapped back at the suggestion that DOs aren’t equivalent to MDs.
Lost in the debate, however, was this:
It wasn’t that long ago that Dr. Conley would not have been permitted to care for the President.
See, Dr. Conley is an officer in the U.S. Navy. And until 1967, osteopathic physicians were banned from practicing in the military.
Matter of fact, it wasn’t until 1969 that the American Medical Association (AMA) even allowed DOs to join. (Until then, the AMA called osteopathic physicians “cultists” and considered any MD who consulted with them to be unethical.)
It’s worth thinking about why osteopathic physicians have gone from a marginalized branch of medicine to one that [intelligent people] consider as having the same skills and qualifications as MDs.
It isn’t because the American public was finally convinced that a well-aligned skeleton was the key to good health, or because the MD-driven medical establishment suddenly became disciples of Andrew Taylor Still’s principles.
Instead, it’s because osteopathic medical schools and osteopathic leadership progressively chose to increase educational standards, better incorporate the scientific foundations of medicine, and emphasized the similarities between DOs and MDs rather than the differences.
Today, we’re gonna take a whirlwind tour through the history of osteopathic medicine, from its humble beginnings on the American frontier to the bustling world of modern residency training, where MDs and DOs work side-by-side interchangeably. We’ll focus generally on the role of licensing and licensing examinations – and by the end, answer the question of whether the National Board of Osteopathic Medical Examiners (NBOME) and their exams are a help or a hindrance to contemporary osteopathic physicians.
–
In the beginning…
When Andrew Taylor Still – the founder of osteopathic medicine – was growing up in the 1800s, medical practice in the United States was very different than it is today.
For one thing, physicians didn’t need a license to practice. Heck, you didn’t even have to go to to medical school – Still himself didn’t. You were a doctor if you said you were. And lots of people said they were.
Franz Mesmer propagated the theory of animal magnetism. James Currie promoted water cures for infectious disease. Sylvester Graham believed that rampant sexual desires caused most maladies and would be cured by eating whole grains and vegetables. There were magnet healers and botanists and hypnotists and homeopaths – and all of them were practicing medicine, at least as the term was then understood.
To some extent, all of these concepts of medicine persist today as alternative therapies. But today, only osteopathic and allopathic doctors are considered physicians.
Why?
–
Increasing standards
It was amidst the proliferation of charlatans and snake oil salesmen that the American Medical Association (AMA) was founded in 1847.
The AMA’s goal was improve the status of physicians and the professional practice of medicine. Toward that end, they created a code of professional ethics and advocated for licensure laws. Now, to be licensed as a physician, you had to at least attend a recognized medical school – no more apprenticeships or proclamations of ability were allowed.
From its beginning, the AMA embraced the scientific practice of medicine. There were lots of ideas about what caused and cured disease – and many of those promoted by MDs were just as laughable as those dreamed up by fringe healers in the 1800s. Still, the principle that medicine was a scientific field – and should be practiced in accordance with the growing scientific understanding of how the universe worked – became firmly established.
Unfortunately, the scientific foundations of medicine were not emphasized by osteopathic medical schools.
When Abraham Flexner visited the flagship school of osteopathic medicine (American School of Osteopathy; now A.T. Still University), he was unimpressed.
[The school’s] entrance requirement [is] less than a common school education.
[Laboratory facilities] are absurdly inadequate for the number of students, as is likewise the teaching staff. . . The dissecting room is foul. The “professors” in charge of histology, pathology, and bacteriology are senior students. . . A course of twenty lectures on the fallacies of medicine is given, so that the graduate will know why he does not use “drugs.”
The school is a business in which a large margin of profit is secured by its owners. The teaching furnished is of the cheapest kind. Its huge income is therefore largely profit.

Waiting room card from Dr. Andrew Taylor Still’s clinic in Kirksville, Missouri, highlighting some of his lesser-known principles (such as “do not talk about your ailments with each other” and “work begins with payment”).
–
Weaponizing licensure
As medicine turned more toward science – and in response to intense lobbying from the AMA – states progressively used their licensure laws as a legal barrier to exclude unscientific practitioners, including DOs.
The lobbying and legislative battles over licensure often turned ugly.
These osteopaths rub backs and desire to have their rubbing legalized.
-A New York State Senator, 1902
(quote from In the Public Trust: The History of NBOME)
–
The bills which the osteopathists have urged through the legislature are examples of the mischief which the leaders of half-baked cults may do in exposing the health of the community to its worst dangers.
–The New York Times, April 5, 1914
–
In the turf war between MDs and DOs, the osteopaths won some battles, earning full practice rights in many states. But each one was a tooth-and-nail struggle against the larger, better-funded, and better politically-connected AMA.
And then, in 1920, the AMA unveiled its new weapon: the basic science law.
These laws required passing an exam covering basic anatomy, physiology, chemistry, and microbiology before the would-be physician could even take the state licensure exam. (Think of it as a pre-modern USMLE Step 1 exam.)
Just in case Flexner’s tone in the quote above didn’t adequately make the point, osteopathic medical schools simply didn’t teach basic science at the level required to pass these exams. (Remember, in the pre-internet era, acquiring scientific medical knowledge meant having access to knowledgeable faculty and/or a good library – both of which were frequently lacking at osteopathic schools.)
The effect of these basic science laws on osteopathic practice were devastating. In Washington, D.C., for example, a grand total of zero DOs were able to pass the basic science test and earn a full medical license.
It didn’t take long for AOA leaders to realize that the practice of osteopathic medicine was in danger of being effectively legislated out of existence.
Unfortunately, political opposition to basic science laws was proving futile. By 1935, seventeen states had these laws in place despite the AOA’s vigorous protests.
If osteopathic medicine were going to survive, they needed a different strategy.
–
If you can’t beat ’em, join ’em
It therefore came to pass that in 1934, in direct response to the proliferation of basic science laws, the AOA voted to make their own licensing examination. The hope was to give DOs a way to become licensed without having to overcome hurdles imposed by the MD-based medical establishment.
The organization that would come to be known as the NBOME was thus created, and in 1936, the first osteopathic licensure examination was administered.
Still, there was a problem: the NBOME had to somehow convince state medical boards to accept the results of their exam. The exam had to be credible, authoritative, and of such quality that states would accept its results as being valid.
And so, they made the wise and calculated decision to focus their exam’s content not on what made osteopathic medicine different – but on what made it similar to the science-based licensing exams already in place.
They mimicked the format of the National Board of Medical Examiners three-part exam series, and although it included osteopathic principles, the exam emphasized the scientific foundations of medicine. The initial written portion did not focus on anything uniquely osteopathic. Rather, the exam had five parts: anatomy, physiology, physiologic chemistry, general pathology, and bacteriology.
Despite their desire to remain different, osteopathic leaders were beginning to realize that there were certain advantages to emphasizing their similarity with MDs.
–
Separate but equal-ish
Gradually, states began to accept the results of the NBOME exam, allowing greater practice opportunities for osteopathic physicians. By the end of the 1950s, sixteen states accepted the NBOME exam in lieu of the state examination. Still, DOs remained marginalized.
For instance, when MDs were drafted into the military during World War II, they served as physicians. When DOs were drafted, they were assigned to serve as medical orderlies or pharmacist technicians.
And although hospitals were desperate for resident physicians – a situation that culminated in the creation of the NRMP Match – most hospitals preferred having unfilled positions to accepting DOs. Instead, most DOs were forced to pursue residency training in osteopathic hospitals.
As time went by, DOs sought greater professional recognition by – you guessed it – again emulating their MD colleagues.
In 1954, the NBME changed its exams to a multiple-choice question format, believing that this allowed more reliable and objective grading. So in 1958, the NBOME followed suit.
And in the 1960s, the AOA began a rigorous accreditation process for osteopathic medical schools – emulating the processes already in place to accredit allopathic schools. The result was a steady increase in the quality of faculty, facilities, and training opportunities at osteopathic medical schools.
By 1973, all states in the United States allowed full practice rights to osteopathic physicians, an achievement that might have been unfathomable to the AOA leaders who fought the AMA in state houses seventy years before.
And as recognition for osteopaths grew, so did the number of osteopathic medical schools.
–
The age of expansion
For most of the 20th century, there were only 5 osteopathic medical schools. But from 1969 to 1978, 9 new schools were added, including publicly-funded schools in Michigan, New Jersey, Ohio, Oklahoma, Texas, and West Virginia.
Another round of expansion in the 1990s and early 2000s created even more schools. By 2010, there were 24 osteopathic medical colleges in the United States.
But expansion was a double-edged sword – because soon, the number of osteopathic graduates began to outstrip the number of available AOA-accredited residency positions available.
In the early 2010s, there were around 7,000 residency positions accredited by the AOA. In contrast, the Accreditation Council on Graduate Medical Education (ACGME) accredited over 117,000 positions. Moreover, most of the AOA positions were small, rural hospitals, some of which were on shaky financial footing. The majority of AOA positions were also in primary care; opportunities for training in medical and surgical subspecialties were scarce.
An increasing number of DO students began to participate in the NRMP Match and compete for ACGME-accredited positions alongside their MD colleagues. But there, they faced steep odds, with Match rates that weren’t much better than graduates of international medical schools.
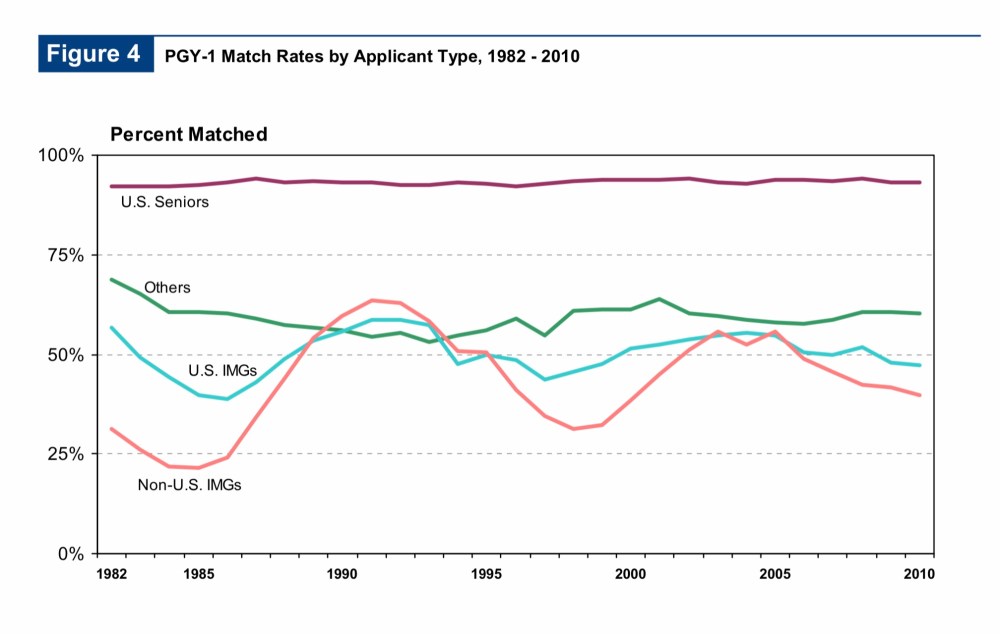
Figure 4 from the 2010 NRMP Main Residency Match report. Until 2019, the NRMP didn’t even include a curve for DOs on this graph, instead counting them among the “others” who applied for residency positions.
Even worse, the ACGME was planning to update their accreditation standards in 2013. Some fellowship program directors had expressed concern about the “heterogeneity” of training programs leading to uneven preparedness among entering fellows, and there was concern that the ACGME’s new standards would end up excluding many DOs from fellowship opportunities.
To ensure the future of the profession, it was clear that the AOA had to act. They needed to ensure access to residency and fellowship positions for DOs, and they knew what they had to do to achieve it.
–
A courageous move
In 2012, the AOA approached the ACGME about a merger.
The ACGME was interested. In fact, they’d discussed this very possibility with AOA representatives at least twice before over the past decade. But the ACGME was negotiating from a position of power, and they knew it. Essentially, they offered to allow AOA programs to apply to for ACGME accreditation. In return, the AOA got to get out of their way.
Many DOs had real concerns about this arrangement. And some osteopathic leaders – like Dr. Norman Gevitz – predicted nothing less than a catastrophe if the merger were allowed to proceed. In a still-famous and highly-influential presentation, Gevitz predicted, among other things, that:
- ~20% of AOA residencies would be unable to meet ACGME standards and would immediately shut down
- Osteopathic residencies would lose their distinctiveness, because MD applicants to AOA programs would sue in federal court if the programs required OMM as a pre-requisite to entry
- Membership in the AOA would plummet, robbing the profession of its political arm
- Osteopathic medical schools would be held to the LCME-accreditation standards used for allopathic schools, resulting in all DO schools being put on probationary status and being forced to cut their class size to 100 students/year or less
- Osteopathic colleges would be required (or would choose) to award the MD degree, eliminating even the term “DO”
- Rural DO schools would become small branch campuses of existing allopathic schools
- Annual DO graduates would decline to 1000-1500/year

To some osteopathic leaders, the AOA-ACGME merger was the first sign of the apocalypse.
In the face of such ominous prophecies, the AOA rejected the original “Memorandum of Understanding” from the ACGME.
Fortunately, wiser osteopathic leadership ultimately prevailed.
By 2014, the AOA and ACGME hammered out a new agreement, giving the ACGME responsibility for all residency programs, while the AOA and AACOM would each get to nominate four members to the ACGME’s 38 person board.
In 2020, the last of the old AOA programs joined the ACGME fold. And in case you hadn’t noticed, Dr. Gevitz’s doomsday scenario did not come to pass.
In the 2020 Match – the first with full participation of osteopathic students – DO seniors had a 90.7% Match rate, not far from the 93.7% enjoyed by fourth-year MD students.
Meanwhile, just this year, two new colleges of osteopathic medicine opened and two others began enrolling students at new branch campuses.
It’s no exaggeration to say that there’s never been a better time in history to be a DO. Today’s students will undoubtedly enjoy brighter prospects for residency training and greater professional opportunities than their predecessors thanks to the courage and circumspection of the AOA and AACOM leadership.
Of course, not all osteopathic organizations have had such foresight.
–
A missed opportunity
In the 1980s, storm clouds were gathering around the National Board of Medical Examiners (NBME).
Since its founding, the NBME had always limited access to their exams to examinees from U.S. medical schools, MDs who went to school overseas instead had to take the Federation Licensing Examination (FLEX). (Some U.S. MDs also chose voluntarily to take the FLEX, because there were a few states that did not recognize the NBME exam.)
However, just to sit for the FLEX, international medical graduates (IMGs) had to take a pre-requisite exam. In 1984, that pre-requisite exam was changed to something called the Foreign Graduate Examination in the Medical Sciences (FGEMS) – which was a product developed by the NBME.
FGEMS was a grueling exam, consisting of 950 multiple-choice questions covering both basic and clinical sciences, taken over a two day period. (Think of it as taking USMLE Step 1 and Step 2 CK on back-to-back days.) For some of the initial FGEMS examinations, fewer than 30% of examinees passed the test.

The old, two pathway examination system for U.S. and foreign-trained MDs. (From this lecture.)
Many IMGs believed that FGEMS was implemented specifically to reduce the number of IMGs entering the U.S. (Sidenote: they were probably right.)
However, this two-test system raised fundamental questions of fairness. If U.S. MDs and IMGs work side-by-side in residency, and are indistinguishable once they’re in practice, why shouldn’t they be held to the same standard of licensure?
State legislatures in California and New York were swayed by this argument, and were poised to enact legislation that would disallow the NBME exams. In response, the NBME began work on a new test, one that would be available to all test-takers regardless of their medical school: the United States Medical Licensing Examination (USMLE).
The NBME and Federation of State Medical Boards reached out to the osteopathic leadership to engage them in the project to make a common licensing standard for all physicians.
No thanks, said the NBOME.
They had bigger aspirations. At the time, they were involved in a messy legal battle to break away from the AOA and become an independent organization. What’s the point of battling for your independence – and then just give up your livelihood voluntarily?
Instead, the NBOME was gonna double down. They’d rebrand their old exams – which had fallen under criticism for their relevance, psychometric validity, and test security – under new name: COMLEX-USA.
To ensure acceptance for their new exam, they went back to the old NBOME playbook – and modeled COMLEX-USA on the USMLE.
The USMLE would be a criterion-referenced test. So, too, would COMLEX-USA. When the USMLE chose to use a three-part series, the NBOME said, hey, us too! When the USMLE began computer-based testing, COMLEX-USA followed close behind. And when the USMLE announced plans to develop a new test of clinical skills – the USMLE Step 2 CS exam – the NBOME raced to follow suit.
Once again, the strategy of mimicry worked.
The Federation of State Medical Boards continued to assert that there should be only one licensing examination for all U.S. physicians, and in 1998, they challenged the validity of COMLEX-USA and demanded a study to demonstrate its worth. But although the review committee expressed some concerns about the COMLEX-USA standard-setting procedure, it was impossible for them to disallow a test that was so similar to their ‘gold standard’ USMLE.
–
COMLEX-USA in the post-USMLE world
By 2005, all states recognized COMLEX-USA for osteopathic physician licensure. And since then, the NBOME’s market position has been secure.
What is less settled, however, is whether we need two pathways for physician licensure.
Through its history, the NBOME has played a useful role in elevating standards and improving the professional standing of osteopathic physicians, using their exams to ensure that licensed DOs were qualified to practice and deserving of the public confidence. In the old days, the very existence of the NBOME and its exams ensured that DOs would not be unfairly excluded from licensure or practice opportunities.
But is that necessary today?
Does having the NBOME help osteopathic physicians? Or is it just an anachronism that’s been allowed to persist due to its monopolistic power? Is the NBOME – in its current configuration – a help or a hindrance to DOs?
If MDs and DOs both take the MCAT to get into medical school… work side-by-side in the same residency programs for residency training… and sit for the same specialty board examinations… why can’t they all take the same licensing exam?
And yes, I’m aware that DOs have a different philosophy and approach to patient care. But the purpose of medical licensure is to protect the public, not codify philosophy. The fundamental elements of safe medical practice are the same, regardless of the philosophy of how they are applied.
And yes, I’m also aware that osteopathic manipulative medicine (OMM) exists, and that some DOs still use it as a part of their practice. To me, that’s a better argument for creating a specific examination in OMM than it is a justification for the NBOME to require all DOs to purchase the store-brand version of a national licensing examination.
Look, I’m not against osteopathic medicine. Truth be told, my own primary care physician is a DO. I count DOs among my most capable colleagues, and eagerly seek out DO applicants for the residency program where I work. I consider DO and MD to be equivalent degrees. But if you want to be sure that the broader public views MDs and DOs as being equal, insisting on a separate measuring stick is foolish.

Quote from In the Public Trust: The History of NBOME. Whose “survival” is Dr. Buser talking about? The survival of the profession – or the survival of the NBOME?
The NBOME has served an important purpose. But DOs should now critically consider whether this is an organization that has largely outlived its usefulness.
In the year 2020, is the NBOME necessary to protect the public or to advance the professional interests of osteopathic physicians? Or does it exist just to feed itself? Has the NBOME become a vestigial organ?
I say it has. And in Part 3, I’ll review the advocacy and policy change necessary to encourage the NBOME to downsize its role. (I’ll also counter some of the objections to my growing belief that the NBOME has become unnecessary – so if you have any, send them in.)
–
YOU MIGHT ALSO LIKE:
Journal Club: COMLEX-USA and Physician Discipline
