
In 1998, a small family medicine residency program in Colorado lost its accreditation.
For the residents at the program, this was a big deal. But it wasn’t the kind of thing that you’d expect to change the course of medical history. And yet, it almost did.
Just like the butterfly who flapped its wings and started a hurricane across the world, this seemingly inconsequential incident set in motion events that would change the history of academic medicine and reach to the highest levels of the U.S. government.
In Parts 1-4 of this series, we learned how the Match came to be. Here, we’ll review how it nearly ended.
–
The Lawyer
After the HealthONE family medicine residency program was shut down, a few of the residents went to see an attorney named Sherman Marek.
The stories they’d told about the working conditions at their residency program were jarring. Like residents elsewhere, they were working virtually unlimited hours for meager pay. But since they’d received their residency position through the Match, they’d accepted their contract sight unseen, without any negotiation over their salary or hours. And because few residency positions were available outside the Match, transferring to another program was difficult if not impossible.
For the first few years of his career, Marek had worked in a firm that specialized in antitrust law. The system the residents were describing didn’t seem like it should be legal.
There must be something I’m missing, Marek thought.
Even after the HealthONE residents’ case was over, Marek couldn’t stop thinking about the strange system that had placed them with their jobs – and removed their ability to negotiate for more salary or better working conditions.
Was the Match legal?
The more he thought about it, Marek didn’t think so.
And soon, he’d get the chance to put it to the test.
–
The Plaintiff
In 2000, Dr. Paul “P.J.” Jung was a fellow at the Johns Hopkins University.
Jung had just finished his internal medicine residency at Cleveland’s MetroHealth Medical Center. As a student and resident, he’d been involved in advocacy and activism. He understood the alphabet soup of medical education and regulation, from the AAMC to the NRMP. And one day, he got a call from an attorney trying to understand those systems a little better.
As Jung taught Marek about the inner workings of the residency placement system, he also learned about antitrust legislation. For over a century, the Sherman Act had made it illegal for cartels to fix prices or suppress competition. And yet it seemed clear that this was exactly what was occurring in residency training.
Jung agreed with Marek. The Match was illegal.
And so, along with two other residents – Luis Llerena and Denise Greene – Jung volunteered to serve as class representatives for all residents in a class action lawsuit against the Match.
Dr. Paul Jung in the New York Times.
–
The Suit
On May 7, 2002, Jung and the other residents filed their lawsuit in the U.S. District Court in Washington, D.C.
Styled as Jung v. AAMC, the suit alleged a conspiracy among the governing authorities in medicine that served to keep resident salaries low and work hours high.
In support of their position, the plaintiffs pointed out several curious things about the resident physician marketplace:
- Resident physicians worked long hours – often 36- or 48-hour shifts. In other industries – that is, in industries in which workers could choose their employer or move freely between jobs – employees seldom (if ever) worked that much.
- Resident salaries were low – at the time, approximately $10/hour. However, residents who worked outside of their residency program – by “moonlighting” in other physician roles – often earned the same hourly rate as an attending physician.
- Resident salaries were stable. In fact, they seemed only to increase at the rate of inflation. If residents were being paid at the market rate, why didn’t salaries fluctuate with market conditions?
- Resident salaries are standardized, regardless of the program quality. In a regular job market, a less-desirable employer might choose to entice workers by offering a higher salary – something that did not occur with residency positions.
- When residency is over, practicing physicians are paid widely varying amounts: a neurosurgeon starts at at a salary around three times that of a pediatrician. Yet all residents are paid the same.
Hmmm.
–
The Conspiracy
To explain these otherwise difficult-to-explain observations, the complaint alleged a three part conspiracy among medical education’s governing bodies.
First up was the Accreditation Council for Graduate Medical Education (ACGME). To practice as a physician, you can’t just graduate medical school. You have to complete at least some portion of a residency. But for a residency program’s training to be considered valid, the residency program has to be accredited by the ACGME. Even the number of positions a program can offer is subject to the ACGME’s approval. There is no alternative system or pathway for a physician to complete their residency training.
Next came the Association of American Medical Colleges (AAMC). At the time, the AAMC – through its Council on Teaching Hospitals and Health Systems or COTH – collected detailed residency salary and benefit data from hospitals, and disseminated those data to its members in an annual report. In some years, the survey even highlighted “atypical” deviations of institutional salaries from the national averages – seemingly a tacit suggestion to not stray from the pack. Once, the survey even inquired whether institutions might support a “uniform schedule” for resident salaries. (Seventy percent of responding institutions answered affirmatively.)
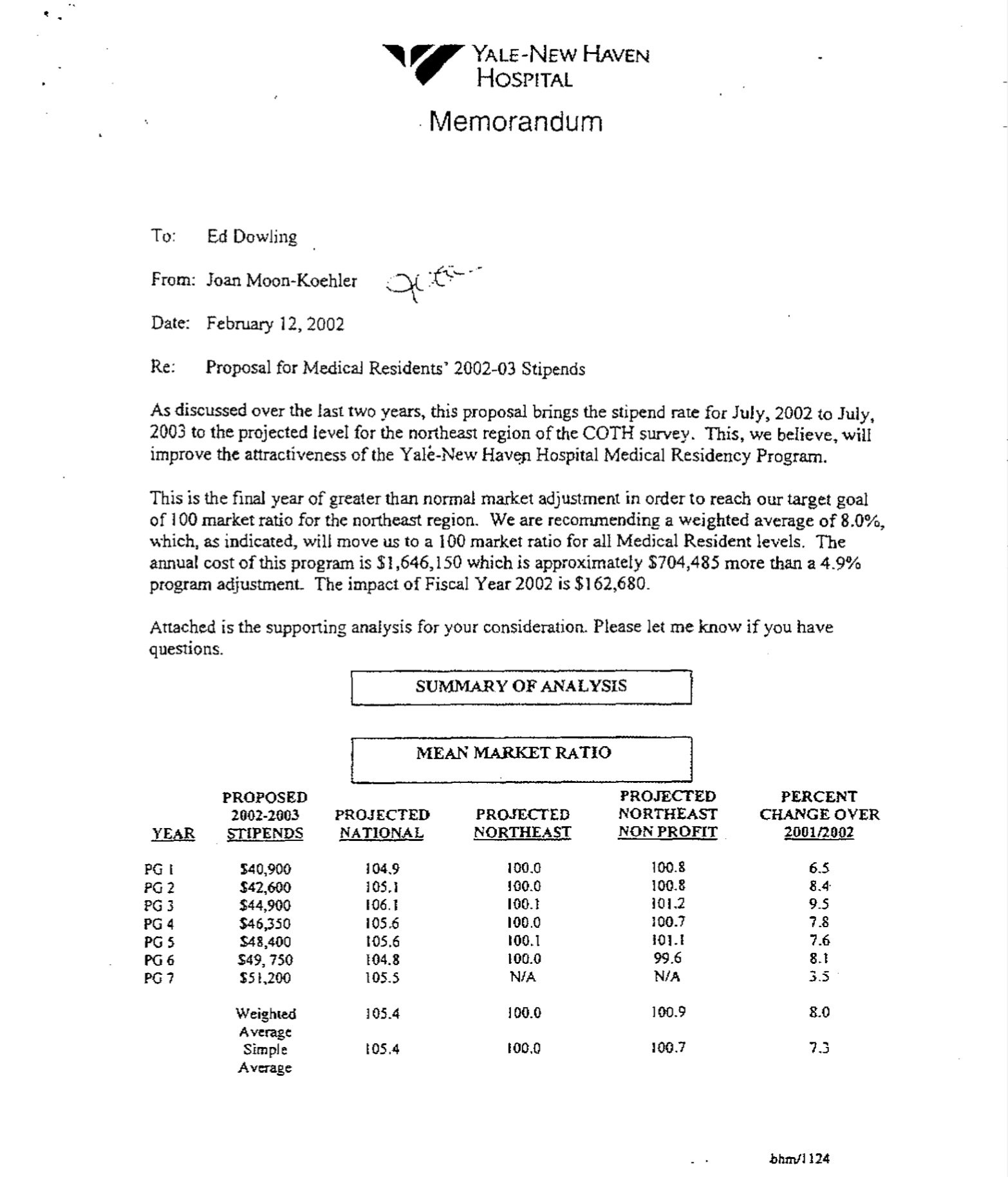
An internal memo from Yale-New Haven Hospital (a defendant in Jung v. AAMC) cited the AAMC’s COTH salary data in setting resident stipends. Note the desire to “improve the attractiveness” of the residency program to applicants… while not being too generous.
The final piece of the conspiracy was the Match. Although the NRMP was not alleged to be directly involved in price fixing, the existence of a matching market was the piece that made it possible.
Because participation in the Match was binding, residents could not hold multiple offers and use that as leverage in negotiations. In fact, the Match ensured there were no negotiations at all. You had to go wherever you were placed (if you were placed), and work the hours that they dictated and receive the pay that they paid.
Taken together, it was easy to see how the ACGME, AAMC, NRMP, and other corporations named in the suit engaged in anticompetitive business practices that were in violation of federal law.
–
The Stakes
Jung v. AAMC went off like a bombshell in the world of medical education – in no small part because the stakes were so high.
The lawsuit was filed on behalf of all resident physicians from 1998-2002 – a class that was estimated to include some 200,000 young doctors. Some simple back-of-the-envelope calculations showed just how enormous the defendants’ exposure could be.
If the court found that the difference between residents’ actual wages and their fair market value was just $15,000 per year, one author conservatively estimated that it would still result in total damages of $3 billion.
Thing is, in antitrust suits, damages are automatically tripled. In other words, if Jung et al. prevailed, the defendants would be on the hook for $9 BILLION.
A judgment like that would be a death blow to the organizational defendants. In 2002, the NRMP took in revenue of only $3.2 million. The relatively well-heeled AAMC had revenues of $56 million that year – a nice chunk of change, to be sure, but nowhere near enough to cover a judgment that size.
But there’s one thing I haven’t yet mentioned: these organizations weren’t the only defendants in the suit.
The suit additionally named as defendants no fewer than 29 hospitals that sponsored residency programs – including giants like Massachusetts General, New York/Presbyterian, Stanford, and Duke.
Including these hospitals as defendants was both necessary and logical for two reasons.
In the first place, although medical education’s alphabet soup organizations might have been responsible for executing the conspiracy that suppressed resident wages, the NRMP and AAMC weren’t the primary financial beneficiaries of these noncompetitive business practices. The hospitals – by enjoying a steady stream of cheap labor – were.
In the second place, for the suit to result in something more than corporate bankruptcies for the AAMC, NRMP, etc., it had to include defendants capable of paying the kind of judgment that the court might return. It had to include the hospitals and their deep pockets.
But deep pockets can also buy powerful allies. Soon, the decision to include the hospitals in the suit would prove portentous.
–
Opening shots
As soon as the suit was filed, all 36 defendants began a vigorous legal defense.
To read through the court records from this time is to take a fully immersive bath in dense legalese. Suffice to say, the papers the parties filed were voluminous. There were motions to dismiss; objections to the court’s jurisdiction; and lengthy answers to the suit. (The NRMP did formulate a unique defense, asserting that the Match participation contract required that disputes be settled in arbitration instead of court.)
Marek was prepared for this. After formulating the case, he’d recruited 16 class action firms to assist with the litigation and keep from getting drowned in paperwork.
But as the depositions and interrogatories and motions built up in one legal skirmish after another, life got increasingly difficult for the residents. Things reached a crescendo in the winter of 2003-2004, prompting the plaintiffs to ask Judge Paul L. Friedman for a protective order.
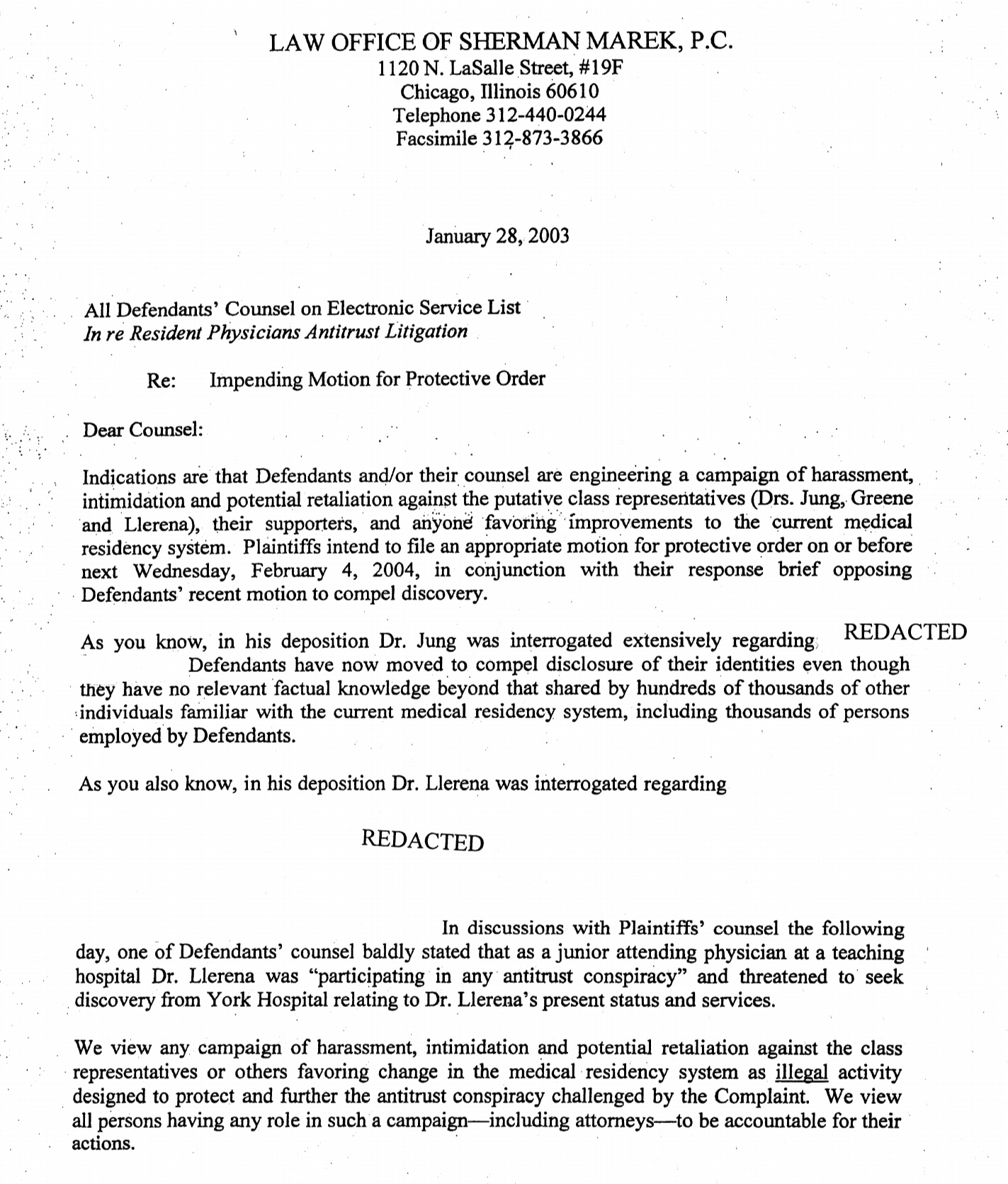
Letter sent by Sherman Marek to the defendants’ attorneys in January 2004 (original mis-dated as 2003).
On February 11, 2004, Judge Friedman made his ruling on the initial motions.
Three defendants – namely, the American Medical Association, the Council on Medical Specialties, and Washington University – saw their motions to dismiss approved, and were released from the case. But for the rest of the defendants – including the NRMP, AAMC, and the vast majority of the institutional defendants – the case would go on.
Dr. Jung was going to get his day in court.
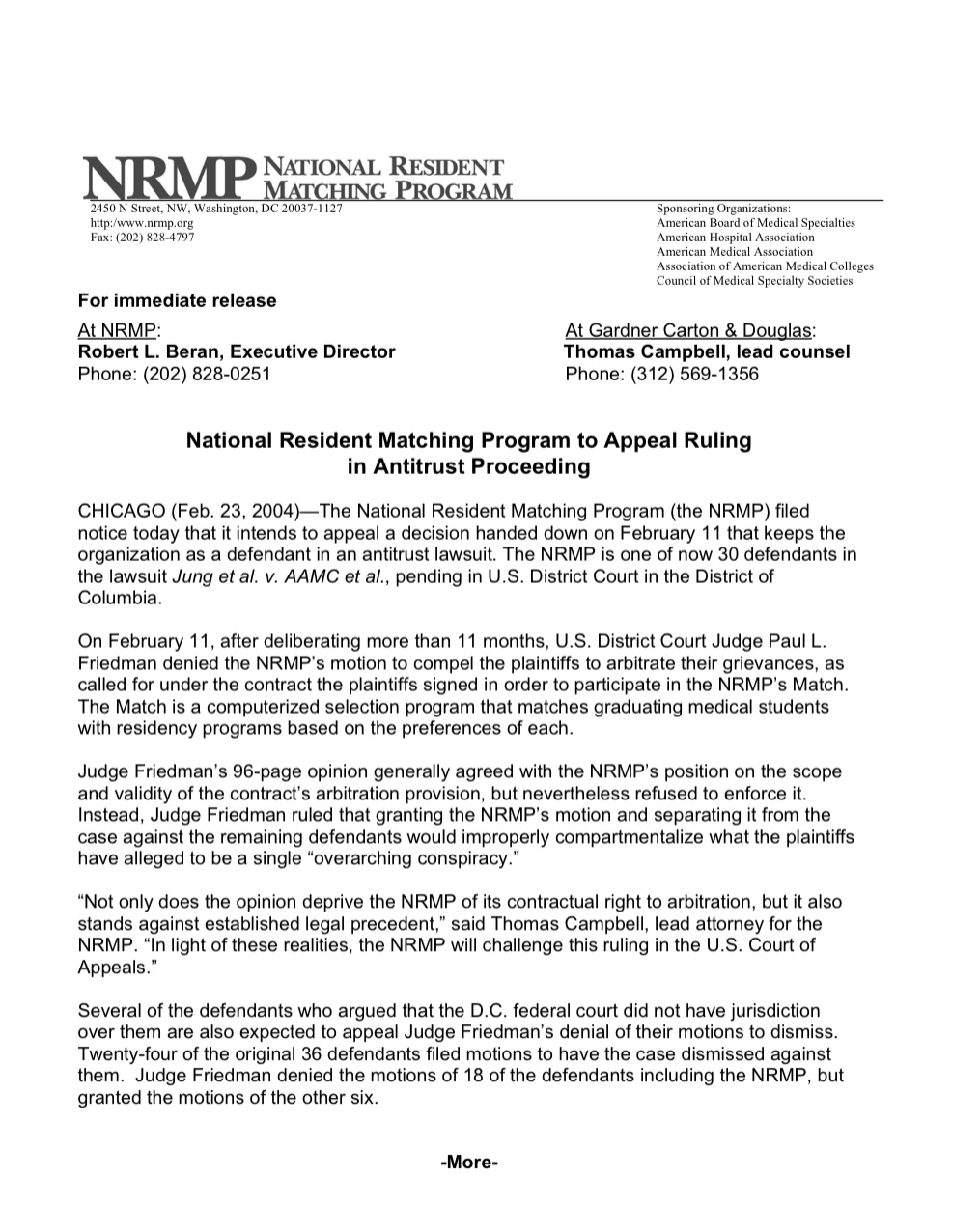
Announcement from the NRMP following the dismissal of their motions, including the motion to have the dispute resolved in arbitration.
–
Damage control
As Jung v. AAMC worked its way through the courts, two other interesting things happened.
The first was the announcement in early 2003 that the ACGME would institute new duty hour requirements. Starting that July, residents would be limited to working 80 hours per week (averaged over four weeks).
Officially, this action had nothing to do with the ACGME’s pending lawsuit. It is true that the ACGME had been studying this issue since the early 1980s… but the final push to implement the duty hour requirements seemed to occur very rapidly, and without any of the administrative flotsam and jetsam that actions of this magnitude typically generate. Based on the historical record (or lack thereof), it’s tempting to speculate that Jung v. AAMC might have pushed this action across the finish line.
It’s easy to imagine why the ACGME and the other defendants might have seen such an action as being beneficial to their case. If, God forbid, the case went to trial, descriptions of resident work hours were likely to generate substantial sympathy from a jury. Maybe the average juror doesn’t have an intuitive sense of antitrust law, but she probably has a strong opinion about whether she wants a resident in the 35th hour of a 36 hour shift performing emergency surgery on her grandmother.
The second development was also telling – especially with the benefit of hindsight.
The defendants – most notably the NRMP – also began a sustained public relations campaign designed to bring more attention to the suit, especially from those in medicine.
Normally, this is not the kind of thing you do when you’ve been accused of orchestrating a vast conspiracy that suppresses wages and leads to inhumane working conditions. But the NRMP and other organizational defendants perceived that the Match was popular, and they sought to leverage that popularity to their advantage.
From the beginning of this lawsuit, the National Resident Matching Program has believed strongly that the plaintiffs do not speak for a majority of medical students or residents.
-Robert L. Beran, PhD, NRMP Executive Director

Screenshot from SaveTheMatch.org, c. 2003-2004. (Link via the WayBack Machine)
See, by the early 2000s, the Match had been in existence for half a century. Essentially every practicing physician had experienced the thrill of opening their letter on Match Day. Some physicians were old enough to remember the bad old days of exploding offers and second-year headhunting by hospitals. (The NRMP’s lawyers actually sought an affidavit from Dr. Hendren, the hero of Part 2 of this series, to show that students had been involved in the original design and implementation of the Match process.)
Thus, through their “Save the Match” campaign, the NRMP sought to make the suit not about whether the Match was illegal – but whether it was good.
Despite the sordid allegations in the lawsuit, most students and residents agreed that the Match should be preserved.
The AMA’s resident and fellow section formally opposed the suit, noting that “dismantling this orderly system without an alternative would be catastrophic for patients and the future of medical education.”
The American Medical Student Association (AMSA) – whose advocacy had been so instrumental in pushing the NRMP to move to an applicant-optimal algorithm – also chose not to support the lawsuit.
AMSA chose to support the NRMP in Jung v. AAMC.
The debate among students and residents on Student Doctor Network similarly revealed genuine uncertainty about what a post-Match world would look like, and whether residents would truly be better off.
Of course, the court cared little about whether SDN avatars like Whiskey Barrel Cortex, orthoguy, or gasman2003 liked the Match or not. The question before the court was whether the conduct and policies of the NRMP, AAMC, and ACGME violated federal antitrust laws. And on that issue, opinion was more uniform: they probably did.
One editorial in the New England Journal of Medicine concluded that “the structure of the Match is anticompetitive, and residents have suffered harm, working long hours at flat salaries,” and opined that the suit had a “reasonable chance of success.”
Legal scholars put the plaintiffs’ likelihood of success even higher.
The plaintiffs have a strong chance at prevailing on their claim that the NRMP is anticompetitive under section one of the Sherman Act. . . Overall, defendants’ possible justifications for the Match appear to be largely policy-based, rather than legally grounded. Even if defendants present strong evidence of the efficiencies created by the NRMP, the court will likely find that such efficiencies can exist within a less restrictive structure.
-Melinda Creasman, Vanderbilt Law Review
So why spend money and effort on increasing public support for the Match? The case was going to be decided based on the law, right?
Right?
–
The end run
So maybe the Match did violate the law. But maybe… maybe the law could be changed.
The AAMC is a trade association. Their job is to advance and protect the interests of medical schools and academic medical centers, and doing so often required effective political lobbying. Their headquarters was in Washington, DC for a reason.
Soon, rumors began to swirl that the AAMC was planning an end run around Marek and Jung’s lawsuit. They would lobby Congress to make an antitrust exemption for the Match.
The New York Times investigated. In an August 2003 story entitled, “Medical Establishment Turns to Powerful Allies to Thwart Residents’ Lawsuit,” the AAMC’s leadership was surprisingly frank about their intentions to have Congress change the law and make all their legal troubles go away.
The article also includes this gem of a quote from the CEO of the AAMC:
It’s precisely because the suit has no merit that we’re going this route.
-Jordan J. Cohen, MD
(Cause, you know, that’s obviously what you do when facing a frivolous lawsuit in which a courtroom victory was assured: call on your powerful friends in Congress to change the law.)
Right around here is where the decision to name individual hospitals as defendants in the suit started to look like a miscalculation.
Academic medical centers are big businesses. They have real constituencies and significant political capital in their home districts. When they speak up, legislators listen.
The hospitals found a particularly receptive audience with Senators Ted Kennedy (D-MA) and Hillary Clinton (D-NY), whose states were collectively home to eight of the hospitals named in the suit. After the defendants hired two former Kennedy staffers, Marek and his team knew they would have to defend their case not only in the courthouse, but also in Congress.
Soon, they found a bipartisan group of senators who were concerned about the backroom deals being made. They were willing to speak out about it – not because it helped their districts, but because it was bad government.
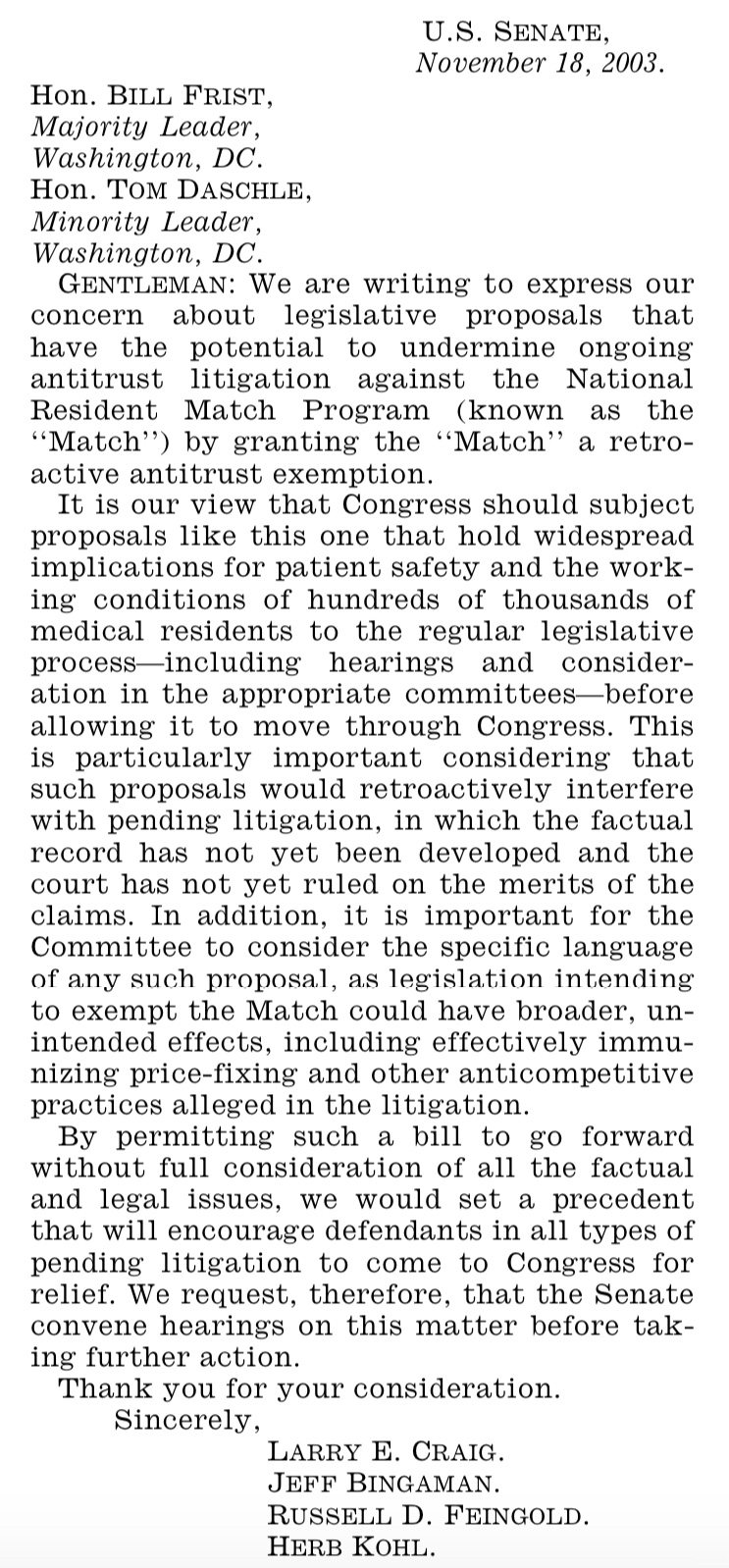
Senators Larry Craig (R-ID), Jeff Bingaman (D-NM), Russ Feingold (D-WI), and Herb Kohl (D-WI) sent a letter arguing that any consideration of an antitrust exemption should be subjected to the scrutiny of the “regular legislative process.”
Marek’s team even hired a D.C. lobbying firm to monitor Congress and sound the alarm if they caught Kennedy or Clinton trying to introduce a bill about the Match.
Problem was, when it mattered most, their watchdog was sleeping.
–
The endgame
In many was, the Pension Funding Equity Act of 2004 is completely mundane piece of legislation. It’s a dreary, technical bill whose principal focus was to change the interest rate used to calculate employee pension contributions.
But when the Senate took up the bill on April 8, 2004, they were under a bit of time pressure. If a new pension funding bill was not approved by April 15, employers would be left without any guidance about how to calculate interest rates for their pension plans. The House had agreed to the Senate version of the bill; now all that was needed was for the Senate to pass it along to the President.
But when the bill came to the floor for a vote, some senators read it and observed that the bill’s sponsors – Senators Kennedy and Judd Gregg (R-NH) – had attached an extra amendment to the bill.
Entitled, “Confirmation of Antitrust Status of Graduate Medical Resident Matching Programs,” the amendment specifically noted that “antitrust laws do not prohibit sponsoring, conducting, or participating in a graduate medical education residency matching program.”
When he took the floor, Senator Feingold criticized the way the amendment had been pushed forward.
I wanted to discuss one additional provision of the bill that has not received much attention in the debate because it was not a part of the bill until just a day or two ago.
I am very troubled by the eleventh hour addition to this conference report of a provision that purports to grant an antitrust exemption to the graduate medical resident matching programs. We have had no hearings on that issue in the Senate Judiciary Committee and no language has ever been presented to the Committee or to the Senate. For the managers of this bill to insert a controversial provision with no Senate debate or discussion is the worst way to legislate, particularly in the complicated area of antitrust law.
-Senator Russ Feingold (D-WI)
Senator Bingaman was similarly scathing in his remarks.
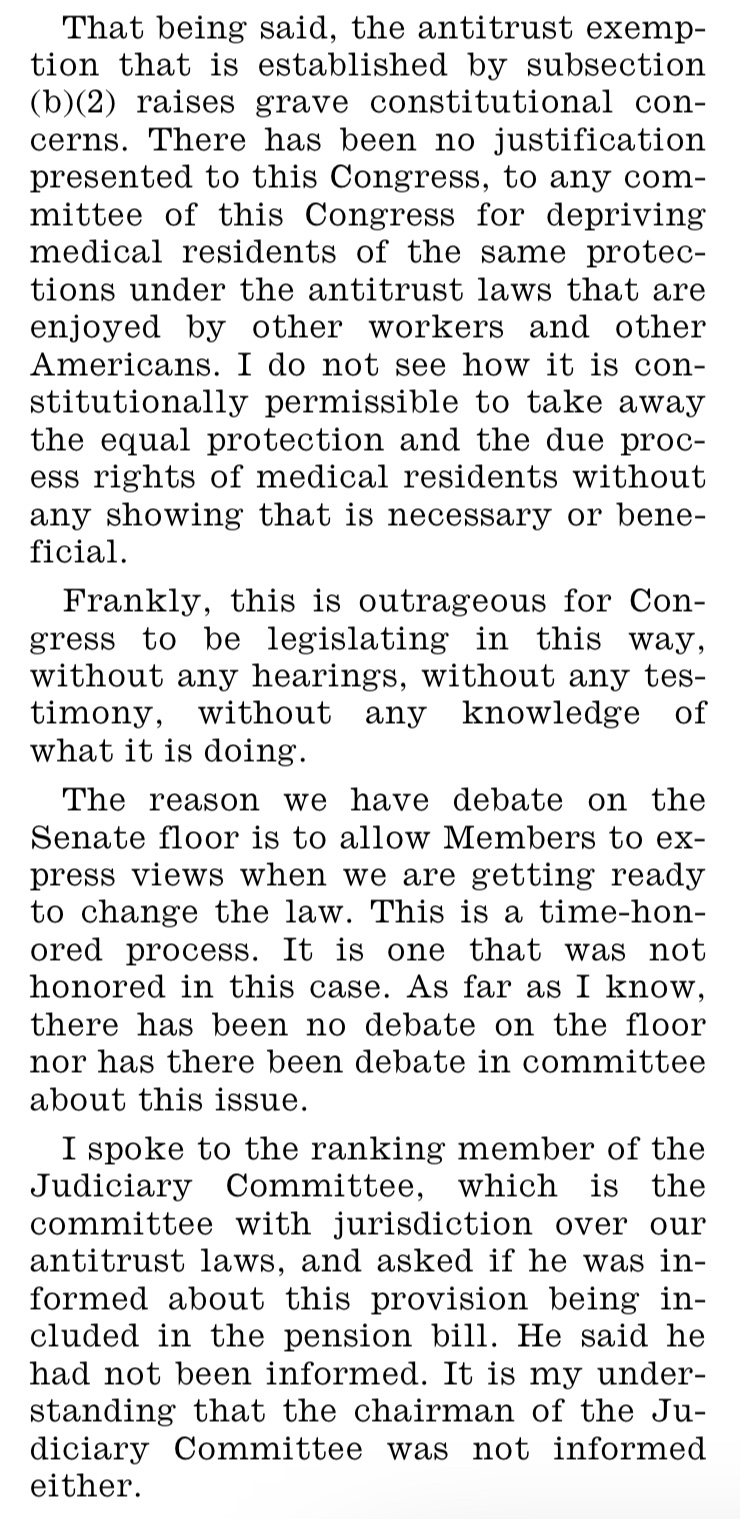
Senator Jeff Bingaman (D-NM), quoted in the April 8, 2004 Congressional Record.
But it was too little, too late. The Senate needed to get this pension business taken care of, and few lawmakers were willing to die on this hill. The measure passed, 78-19. Two days later, President George W. Bush signed it into law.
–
Epilogue
On August 12, 2004, Judge Friedman issued his final order in Jung v. AAMC. Noting that Congress had spoken, he dismissed the suit.
To exempt an industry from antitrust is not without precedent – I mean, look at Major League Baseball – but to bring it about by a clandestine 11th hour amendment without any real debate or broader consideration was decidedly unsavory.
Nearly two decades later, Jung v. AAMC has largely been relegated to a historical footnote, and a largely unsatisfying one at that.
For the defendants in general and the NRMP in particular, the outcome of the suit was a big victory. Although the Match could still unravel, the Pension Funding Equity Act of 2004 secured the NRMP’s legal position for the foreseeable future.
For the plaintiffs, the outcome was a huge loss. Here, it’s worth noting that as class representatives in a class action lawsuit, Drs. Jung, Llerena, and Greene stood to gain no more than any other resident in the class. They didn’t do this to get rich. And after years of serving as the lightning rod for criticism, they walked away with nothing other than a civics lesson and a bitter taste in their mouths.
The plaintiffs’ attorneys were big losers, too. Unlike the defense attorneys – who billed an estimated $500,000 a year to their corporate clients – the firms backing the plaintiffs took the case on contingency. They earned exactly nothing for the untold hours they put in. (For Sherman Marek, at least, there was a silver lining: his leadership established his expertise and launched a career leading one of the few law firms in the country that focuses almost exclusively on legal issues affecting medical students and residents.)
For those not directly involved in the suit, the wins and losses are harder to tally. Though the evidence is circumstantial, I do believe that the implementation of the ACGME’s 80-hour week was at least accelerated by Jung. The lawsuit also led to a new NRMP rule requiring programs to provide a contract to interviewees upon request.
But beyond the winners and losers loomed an unanswered question – the biggest question that Jung raised. Would students and residents be better off without the Match?
Despite two years of legal grappling and political maneuvering, the courts and Congress managed to largely sidestep this question. But I won’t. In Part 6 – the final part of this series – I’ll tackle this question head on.
–
Want a video version of this post to watch, listen, or share with others? There’s one here.
–
YOU MIGHT ALSO LIKE:
The Match, Part 1: Why Do We Have a Match?
Why Do We Have Residency Training?
The Match, Part 3: On Proposals and the Fight for a Student Optimal Match
