One of the fun parts of being in this space is getting communications and questions from readers, social media followers, experts, peers, and people who just stumble onto things I’ve written through Google.
Many of the questions I receive are unique, but there are certain others that I get asked frequently enough that I’ve been slowly posting video responses as a durable resource for everyone. (If you’ve missed that, subscribe to the Sheriff of Sodium YouTube channel.)
And around this time of year, there’s no question I get more frequently than some version of this:
What if I don’t Match?
This is a tough question to answer. In part, that’s because it can be a tough thing to talk about. Many unmatched applicants suffer from intense feelings of shame and failure, and it can be hard to have a frank conversation about strategy and options when you’re managing that grief.
But it’s also a tough question to answer because everyone’s situation is different, and the optimal strategy is circumstance-specific. Still, there are some general themes and advice that apply to all unmatched applicants, and that’s what I’m gonna lay out here. Along the way, I’ll try to highlight some of the broad areas in which the best strategy might differ. Just realize, your mileage may vary.
1. Take care of yourself.
For better or worse, we live in a society in which being a doctor isn’t like other jobs. It isn’t something you do – it’s something you are. And so when you put in the toil and tears to make it up to the final hurdle in medical training – and then stall out – it’s a gut punch.
So my first piece of advice, which supersedes any advice about decision-making or strategy, is to take care of yourself.
Surround yourself with people who truly care about you and filter out everyone else. Get real help if you need it. Take a deep breath and remember that this is not the end.
It may help to remember that you’re not alone. Actually, lots of people go unmatched.
When applicants match at their number one choice, you’re gonna know about it. You’ll see their post on Instagram, #blessed. When people match, they go and tell it on the mountain. When people don’t match, they have a tendency to suffer in silence. You don’t hear from them.
So just know they’re out there – thousands of folks out there, just like you. And perhaps more to the point, there are thousands upon thousands of physicians in current medical practice who initially went unmatched.
But regardless of whether you were shocked to be unmatched or just disappointed, it still sucks. It’s fair to acknowledge that, and you should feel entitled to grieve. But try not to let your grief paralyze you, because you’ve got work to do.
2. Diagnose the problem.
There are lots of reasons why applicants don’t match. And often, applicants know exactly what the reason is in their case.
But sometimes they don’t.
And even if you think you know, my strong advice to you is that you spend at least a few moments to carefully consider whether you have the correct diagnosis – because the reason you went unmatched may influence the strategy you take and the decisions you make.
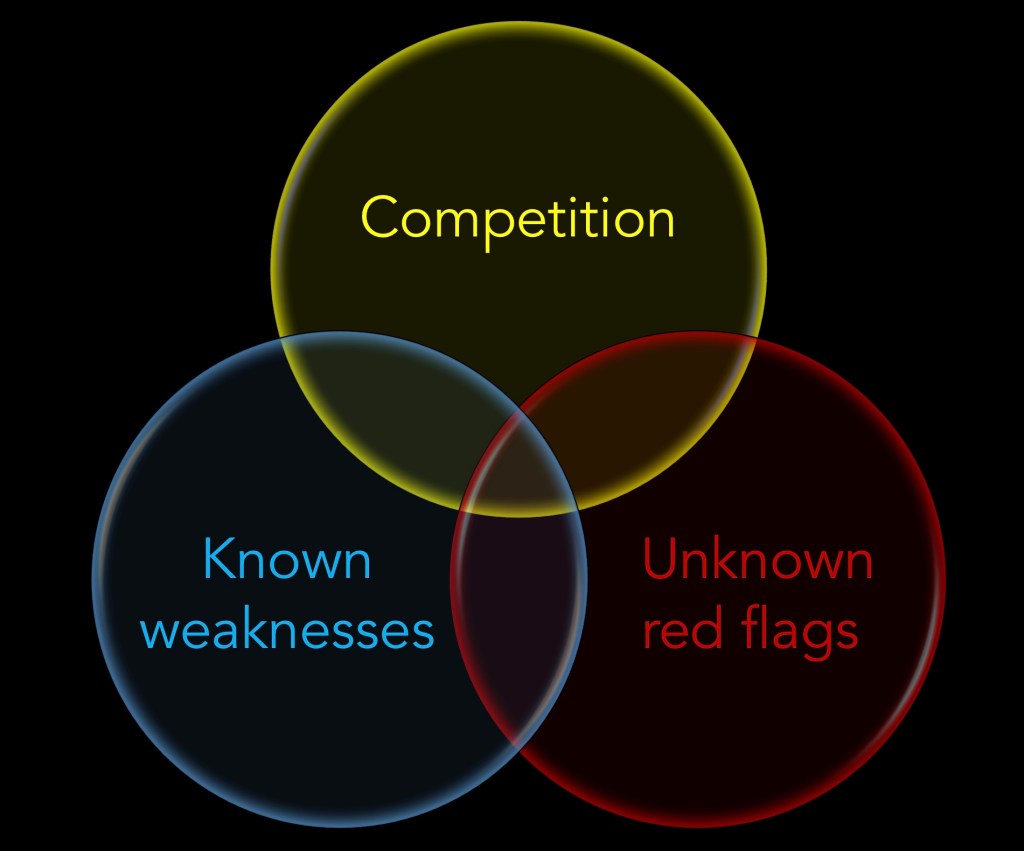
From my standpoint, there are three broad reasons why applicants don’t match.
Please note, these reasons are not mutually exclusive. In fact, they often overlap extensively, and many unmatched applicants have a little of each reason. But it’s still instructive to conceptualize these three broad axes, and you should think about which phenotype best fits you.
–
Competition
The first phenotype is a competitive applicant who applied in a field that was just a little too competitive.
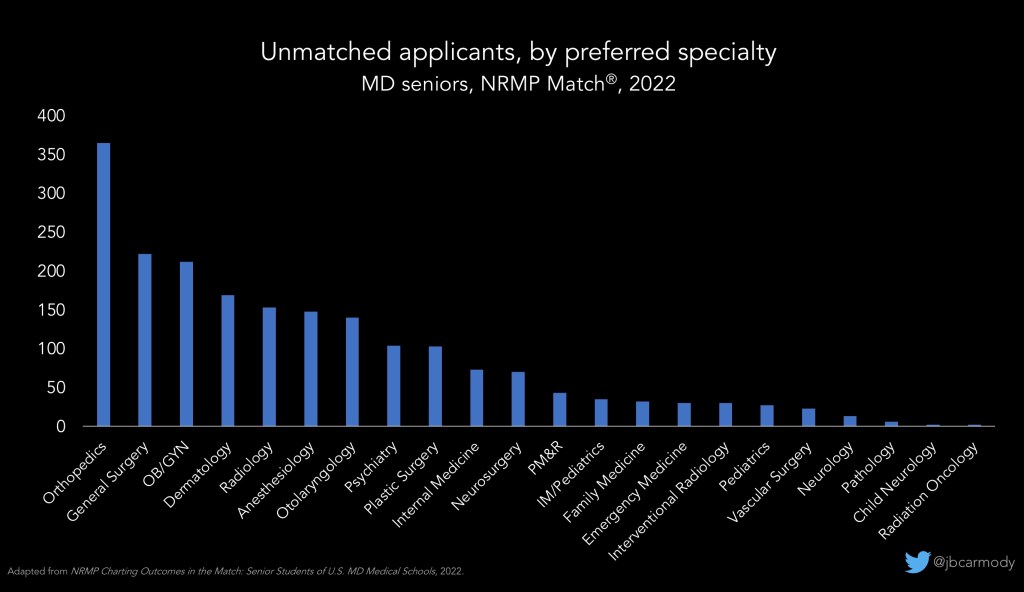
Last year, the Match rate for MD seniors trying to match in dermatology was 72%. For otolaryngology, 69%. For orthopedic surgery, 66%. For plastics, 63%.
I promise you, you’re not gonna find many flaws in the applications of the 30% of applicants who are going unmatched in those highly-competitive specialties. There just happen to be a substantial excess of people with very polished CVs relative to the number of positions available.
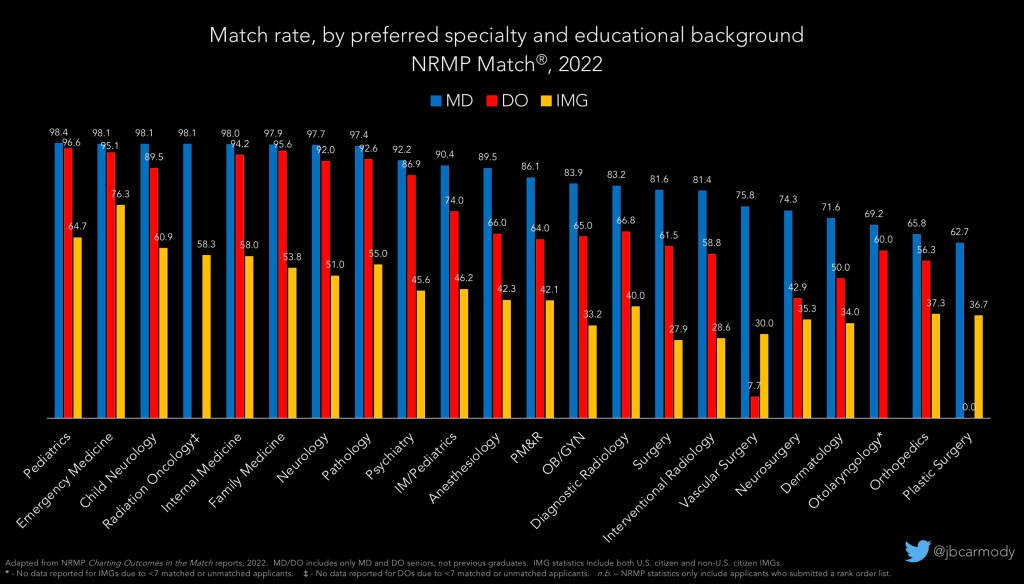
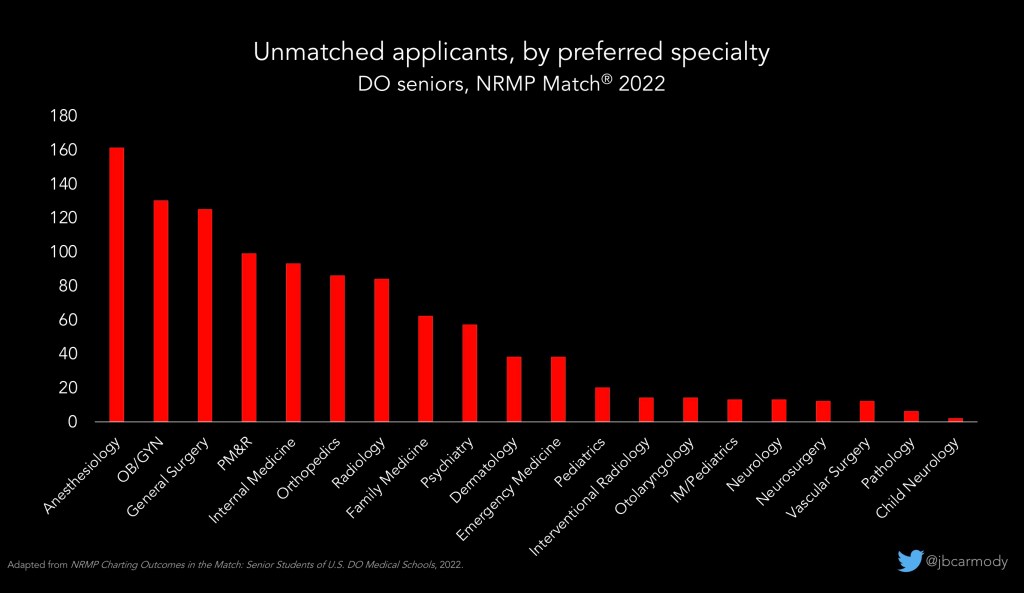
This phenotype also applies to most unmatched DO senior applicants who were applying in anesthesiology or OBGYN or PM&R, specialties for which the match rates were all 65% last year. Again, these are usually strong applicants who probably wouldn’t have had any trouble matching into, say, pediatrics or family medicine. There’s nothing with their application; they were just applying in a competitive field.
–
Known weaknesses
The next category of unmatched applicants are those with what I call “known weaknesses.” This doesn’t mean they’ll be bad doctors. It just means that their application has some weaknesses, and – as my terminology suggests – the applicant knows exactly what they are.
Maybe you failed USMLE. Or you went on academic probation or took a leave of absence. Or maybe you went to a lesser known Caribbean medical school, or maybe you’ve gone unmatched in previous cycles. The point is, there’s something in your application that you can’t change, but that many programs will perceive as a weakness (and move on to the next applicant without giving you a chance to explain or redeem yourself).
Applicants in this category are usually the least surprised when they don’t match. That’s because, typically, they haven’t gotten very many interview offers. Their known weaknesses resulted in their application being screened out (often by automated filters) at the beginning.
–
Unknown weaknesses
The last category of unmatched applicants are those who have weaknesses or red flags in their application… but unlike a Step failiure or leave of absence, the applicant doesn’t know that they’re there. Often, these applicants are the most shocked when they learn they didn’t match, because they did a reasonable number of interviews and everything seemed to be going well.
Most of the time, these are applicants who have interviewed poorly. If you received a good number of interview offers, it tells you that you had the basic qualifications to match at those programs – but for whatever reason, you didn’t shine as brightly on your interview days.
If this is you, don’t feel bad about yourself.
Again, it doesn’t mean you’ll be a bad doctor. But it is a truism in life that the way that you see yourself isn’t necessarily the way that others see you, and you should think honestly and critically about the way you interview to see if there are ways you can present yourself better.
The other thing to consider is whether there’s something in your application that you can’t see that is keeping you from being ranked highly. Here, the most common culprit is something in your letters of recommendation. (That’s especially true if your specialty uses standardized letters of recommendation, where a preceptor that thought you did just fine but doesn’t grade inflate as much as the average letter witer rates you as “average” and it’s taken as a red flag when the program reviews your application carefully for ranking.)
–
The reason it’s helpful to consider which phenotype of unmatched applicant most applies to you is because the optimal strategy for each varies.
For a highly qualified applicant who was trying to match in a highly competitive field, well, you’ve got to figure out how to make yourself even more competitive. Doing a research year may be more likely to get you where you want to be than panicking and scrambling into a PGY-1 only prelim year in the SOAP.
On the other hand, if your application has some known weaknesses, a prelim position may be exactly what you need. Sometimes, program directors worry that applicants whose CV isn’t spotless won’t be able to handle the rigor of residency. And there’s no better way to prove that you can succeed in residency than by, you know, succeeding in residency.
–
3. Consider your options.
Option 1 – The Supplemental Offer and Acceptance Program (SOAP).
If you take all comers, this is the best option for most unmatched applicants, as it offers the possibility of starting residency training in July. But there are still some things you need to know.
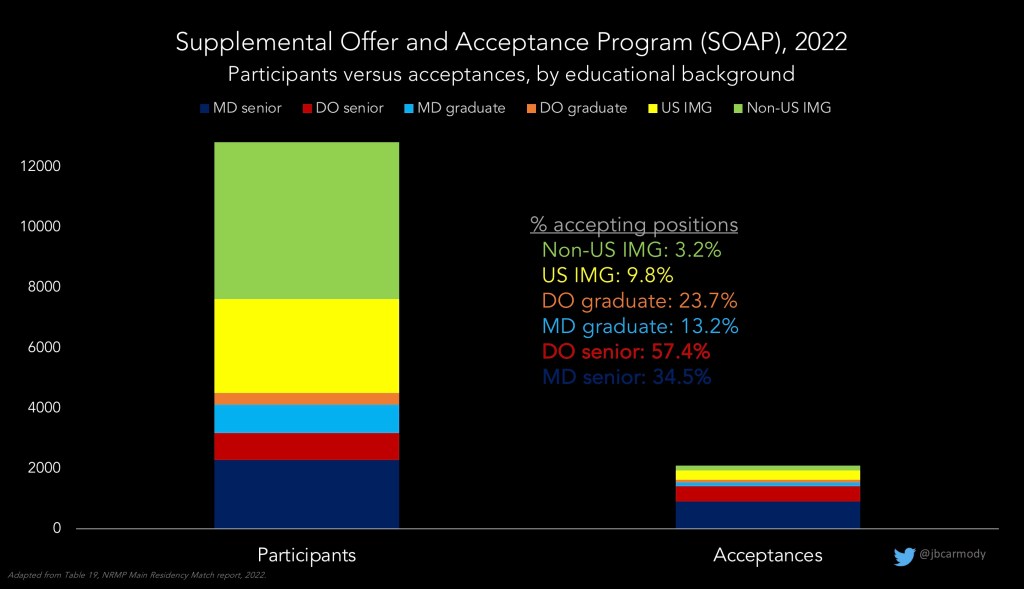
First, you should understand that SOAP is not exactly a buyer’s market. There are way more applicants participating in SOAP than there are positions left over after the Match run.
Second, the type of position available in the SOAP probably isn’t what you were looking for. Although you won’t know the individual programs with positions until Match Week, the general distribution of those positions is pretty consistent year-to-year – and knowing the number and nature of the positions that are likely to be available may impact your decision to participate in SOAP (and if so, what positions you target).
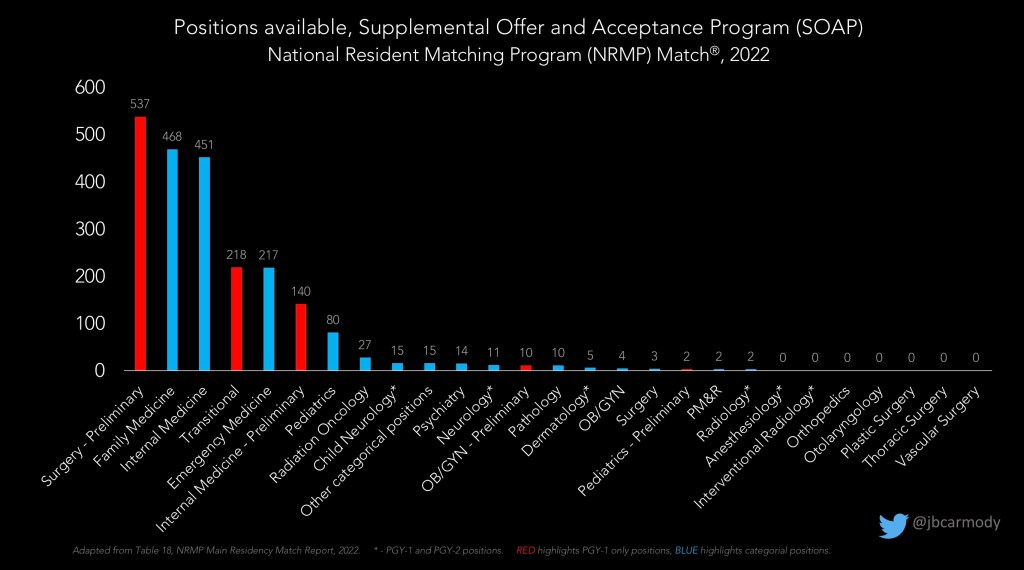
If you went unmatched while trying to get into a highly competitive specialty, there will likely be few – if any – unfilled positions left over in the SOAP.
However, there will likely be several hundred categorical positions in family medicine and internal medicine. Last year, there were 217 emergency medicine positions available, too (and I’ll bet we’ll see significantly more EM positions in the SOAP this year).
Still, around half of the positions available in SOAP are preliminary positions in medicine or surgery or transitional year position. These are PGY-1 only positions. Meaning, if you are offered and accept one of these positions, you’ve got to develop a plan to get into a categorical residency, either through the Match or outside of it, after a year.
For certain applicants, there are potential problems to consider that might arise by accepting a prelim position or categorical position in a specialty other than your ‘dream’ specialty.
Say your dream is to do general surgery, but you accept a preliminary internal medicine position or categorical FM position with the goal of re-applying next year. In the first place, these experiences may not enhance your standing in the eyes of a surgical program director. But more perniciously, they “start the clock” on the funding that the program will receive from the federal government – and limit it to the three years that would be required to achieve board eligibility in IM or FM. This will potentially make it even more difficult – if not impossible – to get a general surgery position later, since the program won’t receive any CMS funding for the additional years needed for surgical training.
The point is, if you choose to SOAP, the first thing you’ve gotta do is clearly define victory. What would a win in the SOAP look like for your situation and career goals?
Some applicants who didn’t match in psychiatry may be just as happy counseling patients in the family medicine clinic. Some wouldn’t.
Some applicants who didn’t match in anesthesiology might be happy doing internal medicine and moving into critical care. Others might be better off doing a surgery prelim year and fighting for a categorical anesthesia position next year.
For applicants with weaker applications, any residency position is better than none. Many applicants who struggle to match for multiple cycles finally get their foot in the door by taking a prelim position. Then, they they seize that opportunity, knock the program director’s socks off by working hard and being reliable, and leverage that to get a categorical position at that program or a strong endorsement to go somewhere else.
The point is, you need to decide whether participating in the SOAP makes sense in your situation, and if so, what types of position would constitute a win.
This is a situation-specific question, and it depends in part what other options you may have available. But if you do choose to SOAP…
i. Clear your calendar.
If you’re a student doing a rotation, you need to be excused. If you’re a prelim resident, you need to be covered as much as you possibly can be. Because things will move quickly, and you need to be prepared to seize any opportunity that presents.
Almost all applicants use the same ERAS application that they used for the regular season. But if you worry that you may have a hidden red flag, it is possible to upload new LORs or a new personal statement – but you’ll have to do it very quickly.
If you’re a student at a reputable school, the preparation for SOAP happen automatically. Your deans may swoop in and help guide you, and you’ll essentially move into a conference room at student affairs until SOAP is over. But for other schools, or for applicants who aren’t in school (or worse yet, are working as prelim year residents) you’ll have to advocate for yourself.
ii. Know the traffic rules.
Because things happen so quickly, and because there are so many applicants and so few positions in SOAP, the NRMP has a few traffic rules that you don’t want to run afoul of.
The most important one is that you can’t contact programs – you have to wait for them to contact you. This rule actually applies to mentors and advisors and anyone else acting on your behalf, too – they’re not allowed to contact programs, either. (In the spirit of honesty, I feel compelled to note that this rule is not always universally observed and that back channel communications – especially among more connected and privileged applicants – do occur. But you should know that it’s a match violation and can be reported to the NRMP, and if you’re the applicant, you’ll be banned from the Match the following year.)
You’re also not allowed to share the list of unfilled programs. In the past, there have been cases where the NRMP has sued entities that shared the program list online.
Another difference between SOAP and the regular application process is that applications are limited. Although there may be 2000 positions available, you can only apply to 45 of them.
This means that the decision about where to submit applications is the most critical decision you’ll make in SOAP week – and you won’t have long to ponder it.
For stronger applicants – like most US MD and DO seniors – make sure that any and all programs you choose to apply to are in line with your definition of victory. For applicants with known red flags who are willing to take any position, don’t waste applications on oversubscribed programs that are just going to screen out your application again. If you are, say, a non-citizen IMG trying to beat the 3% SOAP odds, you need to at least Google every single program you apply to and be confident that they have non-citizen IMG residents before submitting one of your precious applications.
iii. Go all in.
This year, SOAP will consist of 4 individual rounds. You don’t necessarily have to put in all your applications at the beginning… but if your goal is to get a position in the SOAP, my strong advice is that you submit at least 43 or 44 of your applications (if not all 45) in the beginning.
To understand why, put yourself in the program’s shoes. They’ve just spent four months recruiting applicants – and they came up empty-handed. They want those positions filled as soon as possible. If they find someone who is capable and enthusiastic, they’re gonna snap them up, not hope that someone slightly better shows up later. Unsurprisingly, the overwhelming majority of SOAP positions get filled in the first round.
That said, there may be a few of positions that slip through the cracks, and if you have applications left over, you can submit them before the fourth and final round of SOAP. So if you want to hold onto one or two SOAP applications to use as a last minute Hail Mary to an undersubscribed program in Round 4, I won’t be mad at you. But most applicants should go all in to maximize their chance in the first round, and certainly if you hang onto more than 1-2 applications, you’re almost certainly decreasing your chance of coming out with a position (especially a highly desirable one).
If you get an interview, or certainly if you offered a position, my “go all in” advice applies even more. Again, the average program and applicant wants to get SOAP over as soon as possible. If you get a chance, and that chance fits your definition of victory, pounce on it. If you get a bird that lands in your hand, don’t let it fly away while you go rooting around in the bush.
Option 2 – The Research Year.
This may be a good option for competitive applicants who were applying in competitive fields. In fact, an increasing number of incoming residents in ultra-competitive fields like dermatology or otolaryngology have completed a research year – sometimes after initially failing to match.
If you’ve already got a shiny resume but you need to make it more shiny, this may be an option – and for some people it may be a better choice than taking a random position in the SOAP.
Some research positions are just research positions. They’re posted by the mentor or the lab, and they could be filled by anyone. But there are an increasing number of “research fellowships” that are sponsored by residency programs in competitive fields, often at very well-known institutions. They offer research mentorship and some clinical exposure or integration with the residency program, and are marketed to unmatched applicants with the suggestion that participation in their program will lead to success in the next year’s match cycle.
Now, here again, there are some traffic rules you need to be aware of.
Every year, some institutions will advertise their research fellowship positions during Match Week, even though they shouldn’t. Because if you’re a SOAP-eligible applicant, you’re not allowed to take the position if it’s affiliated with a residency program that participated in the Match. So before you sign on the dotted line, you’ll want to make sure that you’re not going to run afoul of the NRMP’s policy.
Option 3 – Delay graduation.
Obviously, this is only an option if you haven’t yet graduated from medical school. But it’s becoming increasingly common for schools to offer an extra year to their students who haven’t matched.
This helps the school in two ways.
For one, even though they usually don’t pay full price, the student still has to pay some tuition for hanging around for that fifth year.
For another, it allows the school to cook the books on their match numbers.
See, most medical schools report their match statistics based on students that are graduating – so if unmatched student gets re-classified into the following class, they get removed from the denominator of the match calculation and the school gets to report a higher match rate.
Of course, taking an extra year can help many students, too. For one thing, it may keep the student from getting screened out by automated ERAS filters in subsequent match cycles.
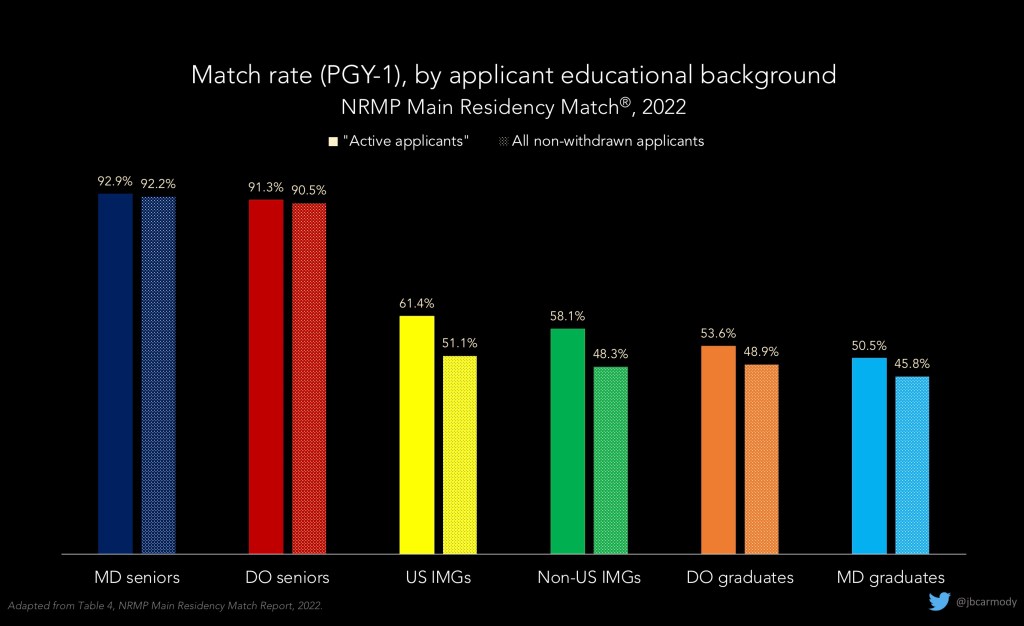
One commonly used filter to screen initial applications in ERAS is the “year of graduation” filter. Many programs choose to limit their reviews to applicants who are graduating that year, or within a couple of recent years. The thinking here is that if someone failed to match in previous cycles, there’s a reason for it. Therefore, PD can either spend the time themselves to scour the application and ferret out what that reason is… or they can just assume that whoever else reviewed the application in previous years knew what they were doing by screening them out or failing to rank them highly.
I’m not saying this is fair or right, but it does occur. Keen eyed viewers may have noticed a few minutes agothat the match rates for graduating MD and DO students were in the 92-93% range, but match rates for previous MD and DO graduates were lower than the match rates for international medical graduates. The reasons for this are multifactorial, but by staying in school, the applicant gets to stay in a more favored category, at least as far as ERAS filters are concerned.
The other potential benefit of staying in school is for students who decide to switch specialties. Some applicants who didn’t match in plastic surgery or orthopedics may be very competitive applicants in, say, anesthesiology or radiology. Someone who didn’t match in OBGYN might be highly sought after in family medicine. But there may be zero (or at least zero desirable) positions available in the SOAP, so these applicants need a year to recalibrate and launch themselves into another field.
And that idea of recalibration – well, that leads into the final possibility that some unmatched applicants may want to consider.
Option 4 – Other options.
I call this “other options” – because the specific option could be a lot of things.
It could be someone who was starting to question whether they had the fire in the belly to do clinical medicine. Maybe their interviewers kind of picked up on that. Maybe that’s why they didn’t match. So maybe now the applicant seizes the opportunity to take their MD and follow their heart and go into some other field. You can’t practice medicine without doing at least an internship, but many doctors have the skills and background to be successful in fields that are adjacent to clinical medicine, like technology or pharma or even administration or business aspects of medicine.
Or it could be someone who desperately wants to practice medicine in the United States, but they got a low USMLE Step 1 score when they took the test 7-8 years ago, and even though they’ve applied and applied, year after year, it’s never happened for them, and now they’re getting fewer interview invites each cycle because they’re getting screened out by Step 1 or year of graduation filters. But maybe they have opportunities to pursue training or to practice in another country, and maybe going unmatched is a sign to shift their course in that direction.
The point here is this: it’s your life.
Many unmatched applicants do not want to do anything other than doggedly pursue their dream in future match cycles. But for others, I want you to know that it’s okay to dream new dreams.
It’s fair to measure the opportunity costs of trying again next year against any and all alternatives available to you. Ultimately, you don’t have to answer to anyone but yourself, and I honestly, deeply believe in my soul that there’s no single true path for almost anyone in this world. The goals we set and the paths we take are the product of so many random things that came before, and physicians could have been put on a different path and been happy and successful and made genuine contributions to the world in other ways. You shouldn’t be afraid to put yourself on a different path and pursue it with just as much passion as you pursued the path that you’d been on. You’ve gotta do what’s right for you.
And that brings me to my final piece of advice, which is this. Once you make your plan, work it. Don’t look back.
It sucks to not match, and I wish it hadn’t happened to you. But this is not the end of your story. All the obstacles you overcame to get here, that all really happened. That was you. All the people who believed in you and saw promise and gave you opportunities, they weren’t wrong. Keep your head up, and take on whatever’s next with grace and dignity.
And remember that I’ll be here cheering for you.
YOU MIGHT ALSO LIKE:
Is there an emergency for emergency medicine?
The Residency Selection Arms Race, Part 3: The Research Arms Race
