The rank order lists were submitted. The button was pressed. And earlier today, 35,984 Match participants learned their fates.
And you know what that means.
Yup, that’s right.
It’s time to break it all down, Winners & Losers™️ style.
–

(Running time 25:08)
–
WINNER: Emergency Medicine.
Last year, the big story was the sudden abundance of unfilled Emergency Medicine positions available in the SOAP. I knew it wouldn’t last.
This year, only 135 positions went unfilled – just 5% of the positions offered – which reflects a substantial drop from last year’s 554 (representing 18% of all positions).

Still, the recovery was uneven.
The number of future EM residents from MD-granting medical schools in the U.S. is essentially the same as last year, and down 27% from its peak in 2021. Fortunately for programs, the number of matched DO applicants is up 43% from last year, and the proportion of total positions filled by international medical graduates (IMGs) hit an all-time hight at 15%.
–
LOSER: Pediatrics.
Don’t say I didn’t warn you.
I told you last year, and again this fall, that the ‘SOAP crisis’ was coming for pediatrics next – and come it did.
This year, 27% of categorical pediatric residency programs went unfilled, while the number of unfilled positions rose to 251, representing a nearly threefold increase from last year.
The sudden increase in unfilled positions has prompted program directors to undertake searching moral inventory, at least on the Association of Pediatric Program Directors listserv.
Was it COVID-19? The ‘tripledemic’? Virtual interviews? A pass/fail Step 1? Programs that didn’t understand preference signaling? The new requirement for pediatric hospitalists to complete a 2-3 year fellowship? Residents choosing to avoid states with restrictions on reproductive health?
Interesting hypotheses, all, but in reality, declining interest in pediatrics among U.S. medical graduates predates all of these things. As a proportion of graduating medical students, pediatrics peaked in the early 2010s at around 10-11% of U.S. MD students and has eroded since, reaching 7.9% in this year’s class. The absolute number of U.S. MDs applying to pediatric residency programs peaked in 2015 and has dropped since.
–
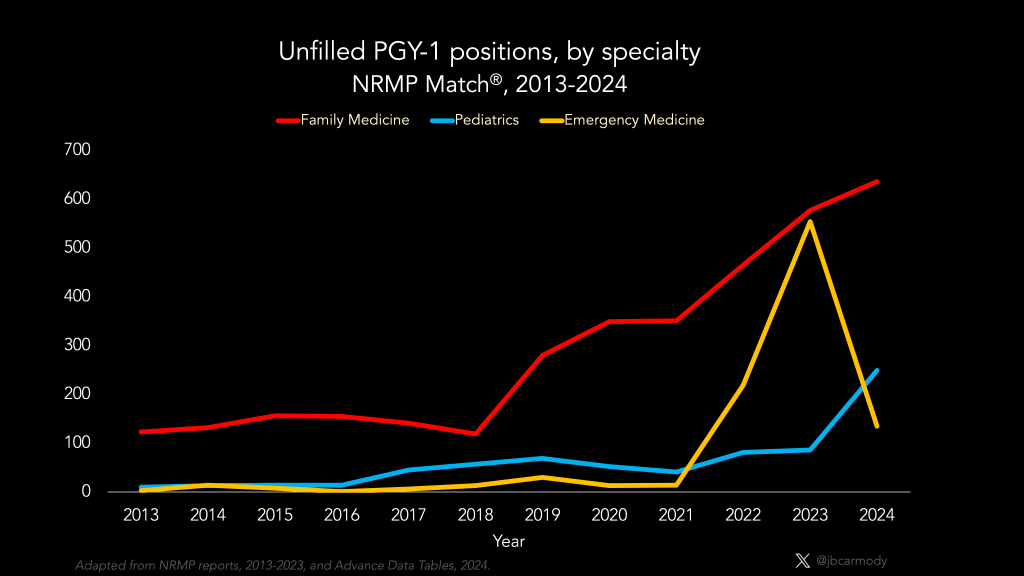
LOSER: Family Medicine.
The specialty with the largest number of unfilled positions was the same as last year, and every other year in recent memory: family medicine. But unlike the media attention given to emergency medicine (2023) or pediatrics (2024) when SOAP numbers suddenly increased, the number of unfilled family medicine positions has been slowly, steadily, and largely quietly building over time.
And just like pediatrics, I’m sure that the reasons for this are complex, deeply nuanced, and multifactorial.
Actually, what am I saying? They’re obviously economic.
Turns out that human beings respond to financial incentives. Given the choice between making more money or less, human beings by and large prefer to make more… and just like everything else in life, you get what you pay for.
–

WINNER: Higher-paying specialties.
If you make a graph plotting the compensation of various medical specialties on one axis, and any measure of ‘competitiveness’ on the other (applicant Match rates, USMLE scores, % of positions filled by U.S. MD graduates, etc.) on the other, I’ll bet you can fit a regression line with a reasonable R2. Higher paying specialties are more sought-after, and this year’s Match data reflect that.
Really, the only surprise for me in the initial NRMP data was anesthesiology. This year, every single one of the 2000 anesthesiology positions filled in the Match. To put that in perspective, plastic surgery, orthopedics, otolaryngology, and dermatology combined also offered ~2000 positions… and there were 7 positions unfilled. (We’ve certainly come a long way from 1996, when only 48% of anesthesiology positions filled in the Match).
Unsurprisingly, orthopedic surgery and neurosurgery appear to have the lowest match rates (~70%, though we won’t know for sure until the NRMP gives us the Charting Outcomes data). Diagnostic radiology seems slightly less sought-after than last year (which means it’s now red hot instead of white hot). Psychiatry remains a challenging match – especially when compared to 10-15 years ago – and both PM&R neurology were competitive and have increased in popularity over the past few application cycles.
–
LOSER: Literal readers.
Every year, after I publish this column, I get messages from a few readers who get madder than a puffed up toad that I said their specialty was a “loser.”
Don’t let this be you.
Winners & Losers™️ is a long-running literary conceit on this website that allows me to highlight tradeoffs or, really, get on my soapbox about whatever I want to talk about. If that doesn’t appeal to you, then please let me refer you to innumerable residency selection hot takes readily-available elsewhere.
The use of this format does not mean that you, personally, are a loser, even if you identify with a category or situation that has been identified as losing in a given scenario. However, if you choose to message me or publicly reply voicing your disgruntledness, you will self-identify as such.
–
LOSER: Workforce conflationists.
During Match Week, you don’t have to look far to find pundits using Match data as a launching pad for their dark prophecies about the looming ‘physician shortage.’
Pediatric positions are unfilled! But who will take care of the children!?!
Hate to burst your bubble, folks, but there are two big problem with using Match fill rates as a measure of anything workforce-related.
First: Those unfilled positions are already filled. We have a SOAP for a reason – and by the time you’re reading this, >95% of those positions are already gone. The few that didn’t will soon be snapped up by eager unmatched applicants in the post-SOAP scramble.
Second – the number of residency positions offered in the Match really has nothing to do with future workforce needs. There’s no physician workforce czar telling hospitals to expand their residency complement in this specialty or that to prevent workforce shortages in the future. Hospitals decide to start a residency program (or expand an existing one) based on their own local economic incentives. There are other factors they could consider, but actually, whether the doctors they train are necessary is perhaps only one they’re specifically prohibited from using in that decision, since doing so might run afoul of anticompetitive business practices or antitrust laws).
–

WINNER: Couples.
One trend I’ve been following in recent Match cycles has been the rise in incomplete couples matches. See, NRMP allows couples to input rank order list selections in which one partner gets matched… and while that’s probably preferable to having both applicants go unmatched, it leads to some Match Day heartbreak and real relationship stress. And last year 9.2% of couples found themselves in such a predicament., which was significantly from 5-10 years ago.
However, this year, the proportion of couples in which only one partner was assigned to a residency program was down to 7.1% – and 90.1% of couples got to share the joy of learning they both matched.
–

PUSH: Dual application.
This year, a record number of applicants applied to multiple specialties. In fact, OBGYN, orthopedic surgery, and urology were the only specialties where less than half of applicants applied to more than one specialty.
Whether this is a good thing or a bad thing depends on where you stand.
For applicants, it’s a mixed bag. Sometimes applying to a backup specialty is necessary, and the fact that the AAMC will let you preference signal as many specialties as you want in ERAS may increase the likelihood of matching for applicants who are savvy in game theory. But of course, dual applying also increases application costs.
For programs, it’s probably more bad than good. Although it’s nice to pick up qualified applicants from other specialties, it’s inefficient and disappointing to spend time interviewing applicants who would prefer to be in another field altogether.
But for the AAMC – sponsor of the Electronic Residency Application Service (ERAS) – dual applying is very good. So good, in fact, that the AAMC officials were miffed that I didn’t leak their dual applicant data when I shared the e-mails they’d sent to deans asking for their help in keeping residency programs from moving away from ERAS.
(And if you want to know why the AAMC cares about this so much… oh boy do I have a video for you.)
–

LOSER: South Asian applicants.
On January 31, 2024, the NBME announced that they were invalidating USMLE scores for >800 examinees who cheated on the exam – many of whom were Match 2024 applicants.
The USMLE’s initial announcement specifically noted that these examinees were “associated with Nepal” – but speculation (and later, the NBME’s own legal filings) – confirmed that the scandal involved other countries, too.
For programs that recruit IMGs, the timing of the announcement (which came out the day before rank order list submission began) and the uncertainty over which applicants might involved, and when programs might learn that they were involved – almost certainly changed ranking decisions.
This week, I heard from numerous applicants from South Asian countries where some examinees had been implicated in the cheating scandal – and they all felt that their applications had suffered because of it. Several of them had done 7-10 internal medicine interviews – and none of them matched.

(From: Charting Outcomes in the Match: International Medical Graduates, 2022.)
Obviously, it’s impossible to know whether these applicants – or others – suffered unfairly because of sharing a country of origin with USMLE cheaters. But it’s hard for me to believe they didn’t.
–
WINNER: DOs.
This year, 92.3% of graduating osteopathic medical students matched – an all-time high. In comparison, graduating MD students had a 93.5% match rate.
Now, it’s true DOs match into a somewhat different distribution of specialties than MD graduates, and DO applicants still face an uphill battle in highly competitive specialties (only 3 DO seniors matched in neurosurgery and plastic surgery, for instance). But the current parity between overall MD and DO match rates is still a truly remarkable trend.
When I graduated from medical school – which I promise, wasn’t that long ago – the match rate for DOs participating in the NRMP Match was 72%. In fact, if you take a look at how match rates have changed for various groups in the NRMP Match over the past 30 plus years, you’ll see that only the DO match rate has changed significantly.

My hope is that numbers like these will finally hush the old-time DOs still whining about the loss of the AOA match and transition to a single residency accreditation system. At this point I can’t see how there’s any debate: today’s DO graduates have much broader opportunities in residency training than their predecessors, and DOs in the future should have brighter prospects still.
–
WINNER: Unmatched IMGs.
Although Match rates for U.S. medical school graduates were high in 2024, IMGs continue to face much longer odds. This year, 67% of U.S. citizen and 58.5% of non-U.S. citizen IMGs matched.
Historically, very few IMGs succeed in the SOAP – last year, just 5.8% of SOAP eligible IMGs got a SOAP position – which would typically mean that the ~6000 unmatched IMGs would be sitting on the sidelines for another year.
But now, that’s changing.
Several states – first Tennessee, then Illinois and Florida – have created pathways to allow some IMGs to bypass residency training altogether. My own state – Virginia – will likely have a similar pathway in the very near future, too. And many other states have passed (or are considering) similar legislation, or have passed other policies that allow IMGs full licensure after less time in residency or create temporary pathways for displaced IMG physicians to practice.

How, exactly, all of these laws will work out isn’t entirely clear. (I gave my initial impression on the Winners & Losers™️ when Tennessee’s law was announced last year. (For now, I’ll simply add that the fact that Tennessee and Florida are both two of the largest states for HCA and two of the first states to pass these laws was hardly surprising.)
But make no mistake: as these laws proliferate, there will be seismic changes in academic medicine, residency training, physician practice, and physician compensation. In the future, we will likely think about this as one of the most important trends in medical training and medical practice to come about in the past several decades. And honestly, most of you still aren’t paying attention.
–
LOSER: Pay-to-play residency training.
All the proposals above are just beginning to come online in 2025, so many unmatched IMGs in 2024 remain desperate for any opportunity to continue their training in the United States. And as usual, the seedy underbelly of the IMG industry is ready to seize the opportunity to make a buck.
This week, I heard from several unmatched applicants with similar stories of being approached by a well-known IMG consulting firm that claimed to have both internal medicine and family medicine positions available for sale.
The price? $150,000 to $200,000.
To find out more details, like the specific position available, the applicants would have been required to sign a non-disclosure agreement.
This wouldn’t be the first time this has happened. If these agreements involve kickbacks to hospitals or bribes to program officials, they’re illegal – and likely will be prosecuted (as they were here).
But even if prosecutors never catch wind of the deal, these things still sometimes go sideways.
One famous example occurred in 2016. It involved an IMG – who had tried unsuccessfully to match in internal medicine, psychiatry, and family medicine programs, and had received a grand total of zero interview invitations after 6 years of applying. But then, his parents were put in touch with someone who made them a remarkable offer. Their son could could have a family medicine residency position – if they could pay $400,000.
So his parents dug deep, and paid the money… and then their son was dismissed from the program within a month of starting.
So you know what his parents did next?
They sued for breach of contract… and ultimately won a $484,000 judgment against the hospital.
(There will be more to come on this story in the future, and I hope we’ll see headlines like some these.)
–
WINNER: USMLE Step 2 CK.
Just over four years ago – on February 13, 2020 – the NBME announced a policy change that seemed, at the time, like it was going to change everything: the USMLE Step 1 exam was going pass/fail.
Well, this was the first application cycle when the vast majority of applicants didn’t have a USMLE Step 1 score. And nothing really seemed different.

From: Mailbag: Questions about the USMLE
I warned when it happened that just making Step 1 pass/fail wouldn’t accomplish much:
Simply getting rid of three digit scores doesn’t improve medical education. And it doesn’t make residency selection any better, either.
It does give us the opportunity to make changes. And the importance of that should not be understated.
Put simply, this is the greatest opportunity for medical education reform since Flexner, and the greatest opportunity to re-design residency selection since… ever.
So did we seize this opportunity? Of course not.
In fairness, it didn’t help that three weeks after the pass/fail announcement, the COVID-19 pandemic truly arrived in the United States, and deans and medical educators and program directors were consumed by finding PPE and making courses virtual and trying to keep themselves and their learners safe and so much other day-to-day chaos that the question of what would come after a scored Step 1 was pretty far down the priority list. And so, collectively, we took the path of least resistance, and just crowned Step 2 CK king.
Here’s the thing about residency selection. We can’t change the number of winners or losers. On Match Day, some applicants will get their dream program. Some won’t. And some will get nothing at all. Unless you can change the distribution of things people want, or the number of those things available, you can’t change the number of winners. You can only change how those winners are determined.
And we can do that in any number of ways. We could use Step 1 scores. Or we could use Step 2 scores. Or we could have a lottery, or draw straws, or just ask people to pay $150,000 for the position they want by directly soliciting them on LinkedIn. We can do it however we want – you’ll have the same number of winners.
But what should be apparent is that the societal benefit – in terms of the quality of doctors we train – will be different under systems. Using Step 2 CK scores is a whole lot better than just having some seedy company auction off positions. But is it the best system we could have? I don’t think so.
We should all want to improve residency selection and the metrics we use. It shouldn’t take a once-in-a-generation change in testing policy to create the desire to have a better system, and that desire shouldn’t be so easily extinguished simply by the availability of convenient alternatives. We should strive to create multiple dimensions of meaningful evaluation that encourage students to acquire real skills that will one day help them help real human patients. What we do in medical education and residency selection matters – and we owe it to our patients to try to do it right.
–
YOU MIGHT ALSO LIKE:
Match Day 2023: Winners & Losers Edition
Match Day 2022: Winners & Losers Edition
