Today, the Coalition for Physician Accountability (CPA) issued their long-awaited preliminary recommendations on the transition from medical school (undergraduate medical education, or UME) to residency (graduate medical education; GME).
For those unaware, the Coalition for Physician Accountability consists of the “alphabet soup” of medical governance organizations (including, among others, the AAMC, AACOM, AOA, AMA, FSMB, NBME, NRMP, etc.).
The recommendations on how to improve the UME-GME transition are expansive, including 42 specific items and running 21 single-spaced pages.
So who wins – and who loses – in the CPA’s recommendations? Yup – it’s time to break it down, Winners & Losers style.
–
WINNER: The Coalition for Physician Accountability.
Two years ago, nobody had heard of the Coalition for Physician Accountability (CPA). Now, they’ve grown into perhaps the most influential body in all of medical education.
Note the word “influential.” The CPA itself has no regulatory authority. Instead, the CPA is kind of like the United Nations of medical governance – and just like the U.N., the CPA’s recommendations carry a lot of weight. Individual schools or programs that choose to go against their recommendations will be swimming against the stream.
Full disclosure, I applied to be on the CPA’s UME-GME committee. I was not surprised when my application was summarily rejected.
So maybe my opinion of the CPA is tinted by a little bit of sour grapes… but from my standpoint, the CPA’s power has grown faster than the trust it’s earned. Yet their UME-GME transition report – and the attention and policy that it will generate – will only solidify the CPA’s newfound central role in medical education.

–
LOSER: Medical students.
The CPA’s committee included 30 members.
Ten were there to represent specific corporate entities (such the the NBME, ECFMG, or AAMC).
Seven were designated as “medical education representatives,” i.e., medical school faculty.
Four were designated institutional officials (DIOs).
Know how many were medical students?
Two.
To be fair, there were just as many medical students involved as there were residents (2), program directors (2), and members of the general public (2). But I still think this sucks.
In my opinion, many of the problems in the UME-GME transition stem from certain organizations working to preserve and maximize their own interests. The fact that the 30 member committee had 10 corporate representatives and a 2/3 majority vote required to pass any recommendation smells a little fishy. So does selecting exactly one MD and exactly one DO student to represent medical student interests on a committee charged with improving the experience of medical students navigating the UME-GME transition.
None of this is to impugn the work of the individuals who served on the committee – who undoubtedly worked diligently and in good faith, and came up with many praiseworthy recommendations. But the composition of a committee tells you something about the values of the organization that convened it – and here, the message is that medical students don’t rate.
–
WINNER: Equity.
At least 6-7 specific recommendations explicitly address equity in the residency selection process, and equitable selection is a dominant theme underlying many of the other recommendations, too.
This isn’t window-dressing, either. There are strong and actionable recommendations including:
- Applicant demographics should be measured and reported in real time (#16)
- Schools must evaluate clerkship grading to evaluate/eliminate systemic bias (#18)
- A database of characteristics of individuals who applied, interviewed, were ranked, and matched at each program should be created and made publicly available (#21)
- Educators must receive faculty development regarding anti-racism (#30)
–
WINNER: The Unmatched.
Unlike most discussions of the UME-GME transition, the CPA report calls for studying the growing number of unmatched physicians – including a root cause analysis and evaluation of disparities.
This is long overdue. Even the scope of the problem itself is unclear. How many unmatched doctors are there? Who knows. And yet, the longer I’ve been in this space, the more I’ve appreciated that we have a real problem on our hands. Saddling some of our best and brightest with $400,000 of student loans when they can’t find a job is a horrific waste of human capital, and serves as a deterrent for future generations of our best and brightest to pursue a medical career.
Most of the simplistic solutions that are often proposed for addressing the problem of the unmatched are childishly naive and have obvious unintended consequences. Kudos to the committee for beginning what I hope will result in nuanced and effective policy solutions.
–

WINNER: COMLEX-USA.
Recommendation #24 calls for the Electronic Residency Application Service (ERAS) to include only a single data field for standardized test scores, which would contain the normalized results of either the COMLEX-USA exam or the USMLE.
In other words, if programs choose to sort applicants by licensing exam scores, applicants will be sorted in order of the percentile score for whichever exam they took – both tests will be treated equally.
If it goes through, this would be good news for osteopathic medical students, who would no longer face the de facto requirement to take the USMLE in order to have their application considered for residency positions.
And it’d be great news for the National Board of Osteopathic Medical Examiners (NBOME), which has faced increasing scrutiny about whether maintaining a ‘separate but equal’ licensing pathway is a good thing for osteopathic physicians. (I say it isn’t.) But if this recommendation is implemented, the COMLEX-USA will live on and the NBOME’s business interests will be protected for the foreseeable future.
(Hmmm… I wonder who was in the committee subgroup who created this recommendation? Looks like the NBOME’s CEO was in the Workgroup B, tasked with evaluating “Mechanics of the Application/Selection Process from the UME Perspective.”)
–
LOSER: Average USMLE test-takers.
The only trouble with reporting a single normalized score for both COMLEX-USA and USMLE is that the USMLE is, on average, a more difficult exam.
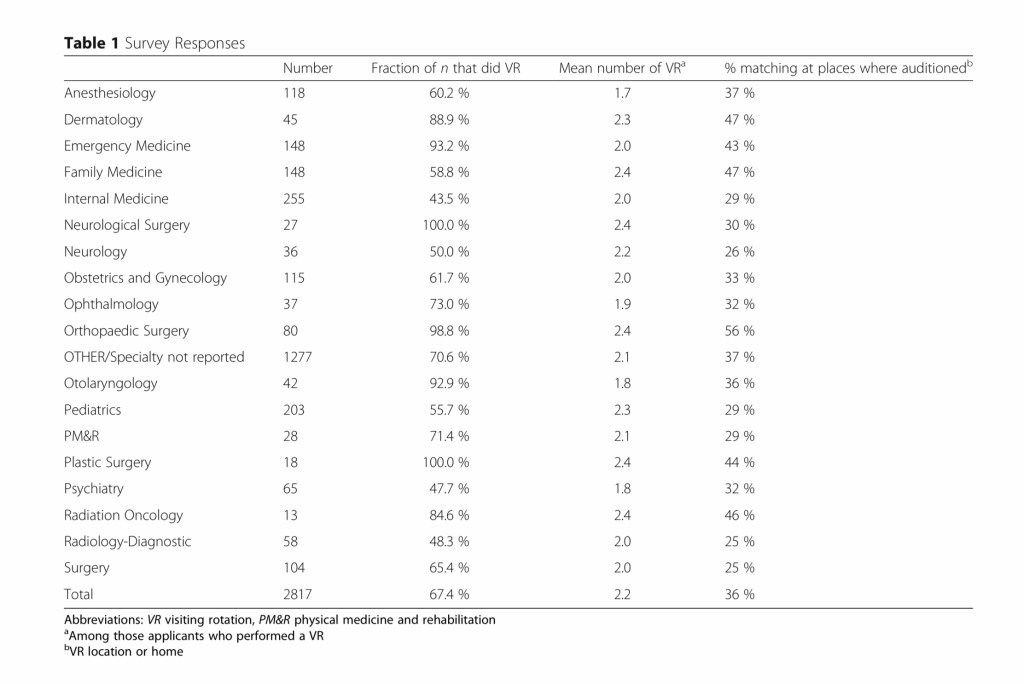
Among osteopathic medical students who took both COMLEX-USA Level 1 and USMLE Step 1, percentile scores are ~20 points lower on the USMLE than on COMLEX-USA.

Put another way, an osteopathic medical student who scores at the 75th percentile on COMLEX-USA would score, on average, around the 50th percentile on the USMLE. Yet this applicant would have the same normalized score in ERAS as an MD or international medical graduate who scored in the 75th percentile on the USMLE.
Look, I’m no fan of using USMLE scores in residency selection, and I’m on record as arguing against the unfairness of DO students having to take two two licensing exams. But to me, a better solution is to eliminate the redundancy, replace the COMLEX-USA with a manipulative medicine exam, and have all physicians take the USMLE.
–
WINNER: Virtual interviews.
Not only does the CPA recommend virtual interviews for the 2021-2022 season, they recommend studying whether virtual interviews should become the permanent means of interviewing for residency.
Hope you invested in that Zoom stock last year, folks.
–
WINNER: Away rotations.
The CPA already recommended limiting away rotations for the upcoming 2021-2022 season (to just one per learner, per specialty). But beyond convening a workgroup to “explore the multiple functions and value of away rotations,” the CPA is silent on the issue of limiting future years’ away rotations.
My guess is that there will eventually be a limitation on the number of away rotations a student can complete. But for now, at least, the possibility of a return to the freewheeling pre-COVID days of away rotations remains in play.
–
LOSER: Application caps.
Despite the assertion that “Application inflation is a root cause of the current dysfunction in the UME-GME transition,” there’s no mention of application caps in the CPA recommendations. (I’m sure the AAMC had their reason$ for not wanting to pursue such a measure.)
Instead, there is a recommendation (#27) for implementing application caps’ weaker but more palatable cousin: interview caps.
Don’t get me wrong – interview caps are a good thing. Eliminating interview hoarding is low hanging fruit that will make things better for everyone. But application caps offer additional advantages – if you can get past the initial knee-jerk “NO!” response.
(Wanna be convinced? Indulge me with a little video).
–
LOSER: PRICE-GOUGED Applicants.
Out of 41 recommendations, exactly zero specifically address the growing cost of the residency application process or call upon the organizations whose revenues are skyrocketing to constrain themselves.
These ostensibly ‘non-profit’ organizations fit the literal definition of a coercive monopoly: students have no choice but to buy their products at whatever to pay whatever price the corporation chooses to charge.
Given the explicit focus on equity elsewhere, this seems like a blind spot. But then you realize that these organizations are the Coalition for Physician Accountability. And then it all makes sense.
–
LOSER: Big Name Letter Writers.
The CPA recommends (#13) that standard letters of recommendation be replaced by structured evaluative letters. These types of letters – also known as standardized letters of evaluation or SLOEs – have been used for several years in certain specialties like emergency medicine (in which they’ve become one of the most impactful metrics used for candidate evaluation).
This is good news for applicants, but not so good news for big-name letter writers whose signature block takes up half the letter page, and who have grown accustomed to a general one paragraph endorsement opening the door to prestigious programs.
–
WINNER: Early Match Proponents.
The CPA gives a special shout-out (Recommendation #28) to early match proposals like the two wave Early Result Acceptance Program. In theory, these programs would function similar to a college early admission program, allowing applicants and programs who are interested in each other to make an earlier commitment (relieving stress for those applicants and congestion for the system.)
These proposals create some tradeoffs… and I have a feeling they may deserve their own special edition of Winners & Losers to analyze them in the future. Stay tuned.
–
LOSER: THE INTERVIEW SCHEDULING FEEDING FRENZY.
Recommendation #25 targets – though not as directly as I might have hoped – one of my most despised application season phenomena: the interview scheduling feeding frenzy.
I’m talking, of course, about the senseless practice of simultaneously inviting, say, 100 applicants to fill 50 interview spots, and scheduling the interviews first-come, first-served.
But curiously, rather than simply insisting on that we eliminate this practice immediately, the CPA calls for the development of a universal interview offering/scheduling platform that would prevent programs from over inviting.
Did you catch that? First we’ll corner the market, then we’ll use our product to force programs to do what we want them to do! (The report doesn’t mention who, exactly, might develop this platform… though at this point it seems appropriate to note the existence of the AAMC’s ERAS interview scheduler.)
–
WINNER: Residency orientation.
Recommendation #34 opines that “residents must be provided with robust orientation and ramp up into their specific program at the start of internship.”
Hey, I like a good orientation just as much as the next guy. And there are some things to which you can’t be oriented until you actually show up. But in an era of limited work hours and increasing resident screen time, opportunities for meaningful patient care and experiential learning are more difficult to come by.
Rather than building up orientation, it might be educationally more efficient if incoming residents showed up on July 1 with more specialty-specific foundational knowledge and skills. Some of that robust orientation might better be transferred to the fourth year of medical school, which for most students is an intellectual wasteland populated by the application process and road to Match Day – and yet is sold at the same price as the educational content delivered in the first three years.
In my opinion, if medical schools don’t provide value commensurate with the price of tuition, they should stop charging so much of it. Either build up practical pre-residency education (Recommendation #33) or discount fourth year tuition.
–
WINNER: Non-clinical DOCTORS.
Recommendation #4 calls for “advising about alternative career pathways” to be available for “individuals who choose not to pursue clinical careers.”
It is true that some students realize only after they’ve entered medical school (and incurred mountains of debt) that taking care of patients is not for them. But my gut says that most of these students would be better served by debt forgiveness and a compassionate off-ramp from medical school than by a school hiring a nonclinical career advisor.
(Expect this recommendation to be especially unpopular at public medical schools. State legislatures may be perfectly happy funding schools that produce doctors to care for their communities – but might be rather less excited about subsidizing the education of hospital executives, management consultants, or entrepreneurs with taxpayer dollars.)
–
Winner: Career-choice changers.
One of the more curious recommendations is #40, in which the CPA recommends that federal funding for residency be counted differently.
At issue is what is called the “initial residency period,” or IRP. The IRP is the period of time for which Medicare will pay the direct GME costs for a particular trainee, and it’s calculated as the minimum number of years of residency training required for board eligibility in the first program at which a resident begins training.
The IRP can issue for residents who realize that they’ve made a mistake in their career choice. Say an internal medicine resident decides she wants to switch to anesthesiology after her intern year. She’s used up one year of the three years of Medicare GME funding for which she’s eligible – so if she finds an anesthesia program willing to take her, she has only two years of Medicare funding left. This funding issue is one reason (among many) that makes it difficult to transfer residency programs.
On the other hand, if the ILP was calculated from the beginning of the second year of residency – as the CPA recommends in their report – it would make it possible for more residents to switch programs after their intern year and still have enough Medicare direct GME funding to get them through their training.
From the CPA’s standpoint, this “will allow career choice reconsideration, leading to [improved] resident well-being” since the initial career choice decision isn’t permanent.
Hmmm.
From my standpoint, a doctor who does an extra year of internship has paid a cost that transcends Medicare funding: they just spent an extra year of their friggin’ life as an intern. I get the point that “students have limited time to definitively establish their specialty choice,” but maybe the best solution to that problem is to provide better career exposure in medical school instead of just financially enabling a costly, soul-crushing mulligan.
–
WINNER: Democracy.
You may disagree with some of the CPA’s recommendations. You might even disagree with my hot takes about them. That’s okay. This is America, and you are free to be wrong.
But since it’s America, you also have the ability to make your voice heard. You have until May 26, 2021 to submit your feedback using this survey.
–
YOU MIGHT ALSO LIKE:
Virtual Interviews: Winners & Losers Edition
The End of USMLE Step 2 CS – Winners & Losers Edition
The Residency Selection Arms Race, Part 2: Anatomy of an Arms Race
